Posted on 02/07/2024 12:05:10 PM PST by Red Badger
One in three Australian adults has high blood pressure (hypertension). Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.
But despite decades of strong recommendations we have failed to get Australians to cut their intake. It's hard for people to change the way they cook, season their food differently, pick low-salt foods off the supermarket shelves and accept a less salty taste.
Now there is a simple and effective solution: potassium-enriched salt. It can be used just like regular salt and most people don't notice any important difference in taste.
Switching to potassium-enriched salt is feasible in a way that cutting salt intake is not. Our new research concludes clinical guidelines for hypertension should give patients clear recommendations to switch.
What is potassium-enriched salt?
Potassium-enriched salts replace some of the sodium chloride that makes up regular salt with potassium chloride. They're also called low-sodium salt, potassium salt, heart salt, mineral salt, or sodium-reduced salt.
Potassium chloride looks the same as sodium chloride and tastes very similar.
Potassium-enriched salt works to lower blood pressure not only because it reduces sodium intake but also because it increases potassium intake. Insufficient potassium, which mostly comes from fruit and vegetables, is another big cause of high blood pressure.
What is the evidence?
We have strong evidence from a randomized trial of 20,995 people that switching to potassium-enriched salt lowers blood pressure and reduces the risks of stroke, heart attacks and early death. The participants had a history of stroke or were 60 years of age or older and had high blood pressure.
An overview of 21 other studies suggests much of the world's population could benefit from potassium-enriched salt.
The World Health Organization's 2023 global report on hypertension highlighted potassium-enriched salt as an "affordable strategy" to reduce blood pressure and prevent cardiovascular events such as strokes.
What should clinical guidelines say?
We teamed up with researchers from the United States, Australia, Japan, South Africa and India to review 32 clinical guidelines for managing high blood pressure across the world. Our findings are published today in the American Heart Association's journal, Hypertension.
We found current guidelines don't give clear and consistent advice on using potassium-enriched salt.
While many guidelines recommend increasing dietary potassium intake, and all refer to reducing sodium intake, only two guidelines – the Chinese and European – recommend using potassium-enriched salt.
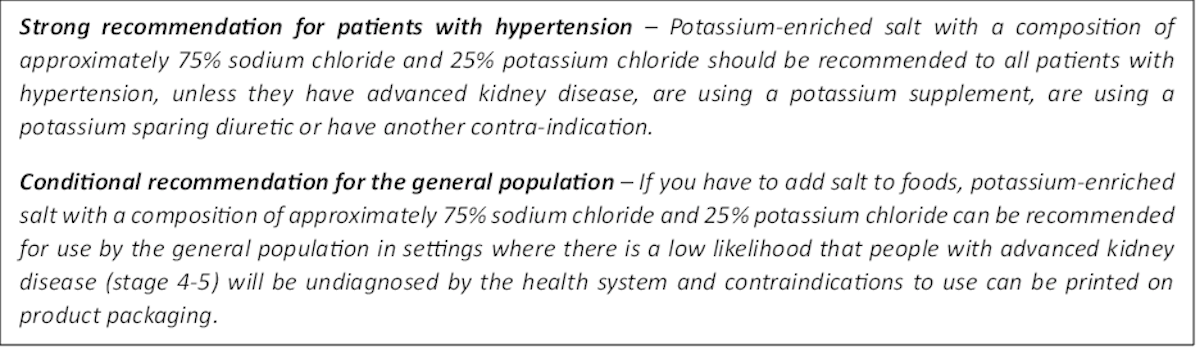
To help guidelines reflect the latest evidence, we suggested specific wording which could be adopted in Australia and around the world:
Suggested guidelines for salt consumption.
Recommended wording for guidance about the use of potassium-enriched salt in clinical management guidelines.
Why do so few people use it?
Most people are unaware of how much salt they eat or the health issues it can cause. Few people know a simple switch to potassium-enriched salt can help lower blood pressure and reduce the risk of a stroke and heart disease.
Limited availability is another challenge. Several Australian retailers stock potassium-enriched salt but there is usually only one brand available, and it is often on the bottom shelf or in a special food aisle.
Potassium-enriched salts also cost more than regular salt, though it's still low cost compared to most other foods, and not as expensive as many fancy salts now available.
A 2021 review found potassium-enriched salts were marketed in only 47 countries and those were mostly high-income countries. Prices ranged from the same as regular salt to almost 15 times greater.
Even though generally more expensive, potassium-enriched salt has the potential to be highly cost effective for disease prevention.
Preventing harm
A frequently raised concern about using potassium-enriched salt is the risk of high blood potassium levels (hyperkalemia) in the approximately 2% of the population with serious kidney disease.
People with serious kidney disease are already advised to avoid regular salt and to avoid foods high in potassium.
No harm from potassium-enriched salt has been recorded in any trial done to date, but all studies were done in a clinical setting with specific guidance for people with kidney disease.
Our current priority is to get people being managed for hypertension to use potassium-enriched salt because health-care providers can advise against its use in people at risk of hyperkalemia.
In some countries, potassium-enriched salt is recommended to the entire community because the potential benefits are so large. A modelling study showed almost half a million strokes and heart attacks would be averted every year in China if the population switched to potassium-enriched salt.
What will happen next?
In 2022, the health minister launched the National Hypertension Taskforce, which aims to improve blood pressure control rates from 32% to 70% by 2030 in Australia.
Potassium-enriched salt can play a key role in achieving this. We are working with the taskforce to update Australian hypertension management guidelines, and to promote the new guidelines to health professionals.
In parallel, we need potassium-enriched salt to be more accessible. We are engaging stakeholders to increase the availability of these products nationwide.
The world has already changed its salt supply once: from regular salt to iodized salt. Iodization efforts began in the 1920s and took the best part of 100 years to achieve traction. Salt iodization is a key public health achievement of the last century preventing goitre (a condition where your thyroid gland grows larger) and enhancing educational outcomes for millions of the poorest children in the world, as iodine is essential for normal growth and brain development.
The next switch to iodized and potassium-enriched salt offers at least the same potential for global health gains. But we need to make it happen in a fraction of the time.
Xiaoyue Xu (Luna), Scientia Lecturer, UNSW Sydney; Alta Schutte, SHARP Professor of Cardiovascular Medicine, UNSW Sydney, and Bruce Neal, Executive Director, George Institute Australia, George Institute for Global Health
This article is republished from The Conversation under a Creative Commons license. Read the original article.
I use Sea Salt in virtually everything that needs seasoning.
My observation is that those that are short of Potassium don’t mind the taste difference. I take medication that tends to deplete my potassium reserves and have to take supplements occasionally. If I am “good” with my potassium levels, the salt substitute is ... underwhelming. If I am low, I can hardly taste the difference.
I am chronically low on potassium.
I take a 2% DV supplement twice a day, eat bananas, broccoli and avocadoes, just to stay ‘within range’.............
Celtic sea salt has less sodium than table salt, plus minerals.
You might try the no-salt type of salts just to see if it is acceptable to you. 2% DV is roughly 50 mg dose. Switching to no-salt is not going to significantly add to that but may be an added boost.
You may be low in other minerals as well. I take Bariatric Advantage Advanced Multi EA vitamins, 1 per day, as my regular multi vitamin. You can get them from Amazon, about $45 for 60 count. If I do not take them, after a couple of days I will get leg cramps when I sleep.
Me too.....................
Canned soup is full of some of the unhealthiest processed/modified ingredients out there. I’ve read numerous articles that it’s one of the unhealthiest things you can eat.
Just call me “Pauline.”
I bake my sourdough bread using only fine Mediterranean Sea Salt.
Of course, a tablespoon in a one pound loaf isn’t very much.
I have a niece who is very slim with high BP, though I don’t know about her carb intake. That could be the culprit.
The article starts with BS: “Excess salt (sodium) increases the risk of high blood pressure so everyone with hypertension is advised to reduce salt in their diet.”
Less than 10% of the population is sodium sensitive. For the rest of us it doesn’t matter how much sodium we consume or how much gets replaced with potassium.
For me the solution to high blood pressure was a low carb diet. I can tell when I have been eating too many carbs. My blood pressure shows a direct cause/effect relationship. It will trend higher day by day when I don’t control carbs. Get myself back into proper ketosis and my blood pressure goes right down again, no meds needed.
If you are part of that tiny part of the population that is actually sodium sensitive, then do it. For the rest of us it doesn’t really matter. Insulin resistance is more commonly the root cause of elevated blood pressure.
I was put on a low sodium diet 18 months ago due to a Pulmonary Edema attack. Thought I was going to die. They said 2000 mg/day. I keep mine almost daily at or under 1500.
Prior to Edema attack my BP was routinely 140/100 sometimes less for decades. Now I check weight n BP daily, I’m slowing losing weight and BP is never over 120/80 usually 100+/60+.
The best indicator of my sodium level are my ankles, water retention ie puffy ankles.
Should have changed 20+ years ago, BUT ... didn’t heed Dr warnings.
Near death is a great motivator
Forgot to mention, virtually anything in a box or can is high sodium.
Weight loss can help with BP.
Agree completely.
About a year ago, I started taking a Ca-Mg-Zn supplement for my bones and to help with sleeping, and I rarely have leg cramps anymore. I’m guessing it’s the magnesium but not sure.
Your daily diet needs some salt. But if you like a lot of snack foods, and other salty foods, you can take in took much salt, no matter if you have hypertension or not.
The trick is not to eliminate salt, just not overdo it.
As to who can overdo it even while watching their salt, there are some individuals who have a problem with the adrenal glands, which is sending out false signals telling the system to retain excess salt above what is needed. Someone can have a good artery and vein system and still have hypertension just due to the problem I just mentioned.
I do watch salt on store bought foods and keep away from any item where the salt content per serving is greater than 1/3 the daily salt requirement.
I do not add much salt in cooking. But the other day, being very good with my salt intake, I had a craving for salt, which I honored with a salty snack. Strangely an hour and half later my blood pressure had gone DOWN a good bit.
I watch the salt but I don’t worry a ton about it.
I think salt concerns as far as hypertension can actually vary with the individual and there may be genetic differences regarding how well, or not, we process and/or retain salt.
Sooner or later getting medical practice will include using our own genetic code, analyzed and fitting our gene expressions to what medicines are needed or not needed for us, as an individual, as well as which ones are best for us, or to be avoided with us.
There are now two major studies, one with a million participants in the Veterans Administration health system, which are making exactly those kind of studies. The VA calls theirs the MVP (Million Veterans Program). It looks at how genetics as well as lifestyle and military experience may influence health care practices for an individual.
My BMI is 22.3. I can’t lose much more without losing muscle. BP is excellent as long as I don’t go crazy with the carbs. Got to the edge of prehypertensive with splurges around the holidays but came back down nicely when I got back on track.
Carbs are the problem, not sodium. And not weight in my case.
I have found that low-sodium V-8 (the Tomato-ey vegetable juice) has 1250mg of potassium (25% dv) in the 11.5 oz can, and only 200 mg sodium. I also just bought 3.5 lb of prunes for $9.99 @ Costco.
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.