. . . . . . . . .
Posted on 11/19/2022 12:07:42 PM PST by Bob Ireland
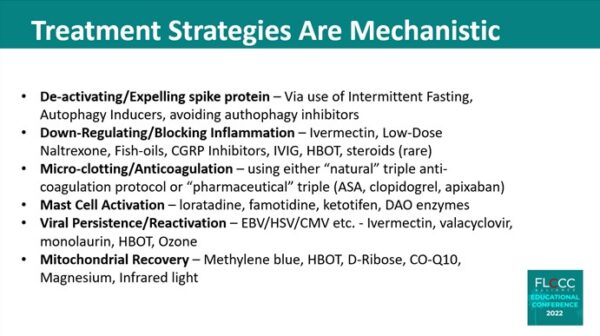
“Post-COVID-19 vaccines syndrome,” said Dr. Paul Marik, co-founder and Chief Science Officer of the Frontline COVID-19 Critical Care Alliance (FLCCC), on Oct. 15 at a conference in Orlando, Florida, aimed at education and sharing information on treating spike protein-induced health issues.
Marik and 15 other experts including pathologist Dr. Ryan Cole, FLCCC co-founder Dr. Pierre Kory, and Steve Kirsch, founder of the Vaccine Safety Research Foundation, presented their research and findings.
. . . . . . . . .
Why would you want to discuss anything in private with someone you imagine is “trolling” you?
You publicly claim I am “off focus” but do not want to publicly say what you mean by that.
If there is something very wrong, why does it have to be someone else’s fault? What about your contribution? Do you think you are perfect and infallible?
I told you I would not discuss this privately. Please honor that and stop with the private messages Say what you have to say out in the open and publicly.
I was taking plenty of d, c, zinc and quercetin in May. I went to a 3 day music festival. Afterwards, I got covid. (2nd time) my only symptom was crushing fatigue. For about a week. I’m sure my healthy supplemented body kept it from being worse. We will all be exposed to pretty much all the viruses. Prevention is the best way to get a lesser case.
I-RECOVER
Post-Vaccine Treatment Protocol
Management of Post-Vaccine Syndrome
Major public health authorities do not recognize post-COVID-vaccine injuries and no specific ICD classification code exists for this disease. However, while no official definition exists, a temporal correlation between receiving a COVID-19 vaccine and the beginning or worsening of a patient’s clinical manifestations is sufficient to diagnose a COVID-19 vaccine-induced injury, when symptoms are otherwise unexplained by concurrent causes.
Since there are no published reports detailing how to manage vaccine-injured patients, our treatment approach is based on the postulated pathogenetic mechanism, clinical observation, and patient anecdotes. Treatment must be individualized according to each patient’s presenting symptoms and disease syndromes. Chances are, not all patients will respond equally to the same intervention; a particular intervention may be life-saving for one patient and completely ineffective for another.
Early treatment is essential; the response to treatment will most likely be attenuated when treatment is delayed.
First Line Therapies
Intermittent daily fasting
. . . . . . . . .
Ivermectin: 0.2-0.3 mg/kg/day
. . . . . . . . .
Moderating physical activity
. . . . . . . . .
Low Dose Naltrexone (LDN)
. . . . . . . . .
Resveratrol
. . . . . . . . .
Melatonin: 2–6 mg slow release/extended release prior to bedtime
. . . . . . . . .
Aspirin: 81 mg/day
Probiotics/prebiotics
. . . . . . . . .
Sunlight and Photobiomodulation (PBM)
Adjunctive/Second-Line Therapies (Listed in order of importance)
{MORE ...}
©2020–2022 All Rights Reserved FLCCC Alliance
pdf’s available for download with previous.
“VAERS - Virus Adverse Effect Reporting System. :) The system had come under increased criticism, apparently for political reasons. “
VAERS isn’t under attack at all. It was created by the CDC and they continue to use it.
The criticism has been of people who are using VAERS data as if the reports are verified when none of them are. Anyone can file a VAERS report, no one verifies them before they are posted.
The VAERS site itself says what the system is designed to do:
“VAERS is a passive reporting system, meaning it relies on individuals to send in reports of their experiences to CDC and FDA. VAERS is not designed to determine if a vaccine caused a health problem, but is especially useful for detecting unusual or unexpected patterns of adverse event reporting that might indicate a possible safety problem with a vaccine. This way, VAERS can provide CDC and FDA with valuable information that additional work and evaluation is necessary to further assess a possible safety concern.”
https://vaers.hhs.gov/about.html
Thanks.
BKMK
3. Ivermectin for Long COVID and Post-Vaccine SymptomsThe number of studies supporting ivermectin to treat long COVID and post-COVID-19 vaccine symptoms is limited. However, doctors treating these conditions have observed successful results with ivermectin.
An Argentinian study published in March 2021 is the only peer-reviewed study evaluating ivermectin for long COVID.
Researchers found that in patients reporting long COVID symptoms—including coughing, brain fog, headaches, and fatigue—ivermectin alleviated their symptoms.
Mechanistically, ivermectin can improve autophagy {which see}. This process is usually switched off during COVID-19 infections. By switching autophagy back on, ivermectin can help cells clear remnant viral proteins out, returning stability to the cell.
Like acute and severe COVID-19, chronic spike protein triggers inflammation, and ivermectin can reduce such responses by suppressing inflammatory pathways and lessening the damage to tissues and blood vessels.
This article, written by Marina Zhang, is based on research by the Front Line COVID-19 Critical Care Alliance (FLCCC) and Doctors Paul Marik and Pierre Kory. The whole article is informative concerning the development of ivermectin and its increasing usefulness globally. The drugs developers in 2015 received the Nobel Prize in Physiology or Medicine. The World Health Organization has listed ivermectin as an essential drug.
You might consider some of the post-CoViD treatment suggestions offered here just to head off any unforeseen long term effects. You were taking OTC meds prophylactically prior to infection; there are some good offerings listed here, e.g. resveratrol, CoQ10 and magnesium, good antioxidants that might help promote autophagy - the process of cleaning out CoViD remnants from the individual cells and restoring them.
Immunity might be strengthened with loratadine {Claritin} and famotidine {Pepcid}. 🤔
To thepoodlebites: Is this the study you remember? Full version here:
https://www.biorxiv.org/content/10.1101/2020.01.30.927871v1.full
___
That’s it, I specifically remember the colorful illustrations in Figure 3. Thank you so much. Knowing what we know now, that the SARS-CoV-2 virus shows evidence of bioengineering and most likely escaped from the Wuhan Institute of Virology, this pre-print represents valid work that was done soon after the Covid-19 outbreak but was subsequently pulled by the powers-that-be.
From the paper:
We found four new insertions in the protein of 2019-nCoV- “GTNGTKR” (IS1), “HKNNKS” (IS2), “GDSSSG” (IS3) and “QTNSPRRA” (IS4) (Figure 2). To our surprise, these sequence insertions were not only absent in S protein of SARS but were also not observed in any other member of the Coronaviridae family (Supplementary figure). This is startling as it is quite unlikely for a virus to have acquired such unique insertions naturally in a short duration of time.
You are most welcome, but the credit goes to Pelham (see #115). I’ve always thought it was leaked from that leaky Wuhan lab. Compelling evidence here:
https://thebulletin.org/2021/05/the-origin-of-covid-did-people-or-nature-open-pandoras-box-at-wuhan/
BTTT
* * * C-19 Thread / FLCCC / Treatments to counter mRNA spike-protein damage * * *
Got info from here, posted on twitter. Thanks for the thread.
That's great news! Thanks, lj! :^)
bkmk
BTTT
For more study bump - COVID-19 Vaccine Injury - Treatments to Counter mRNA Spike Protein Damage
BTTT
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.