Posted on 05/10/2025 7:07:23 AM PDT by Red Badger
Paediatric gender dysphoria has rapidly emerged as one of the most divisive and urgent issues in medicine today. In the past decade, the number of children and adolescents identifying as transgender or nonbinary has soared.
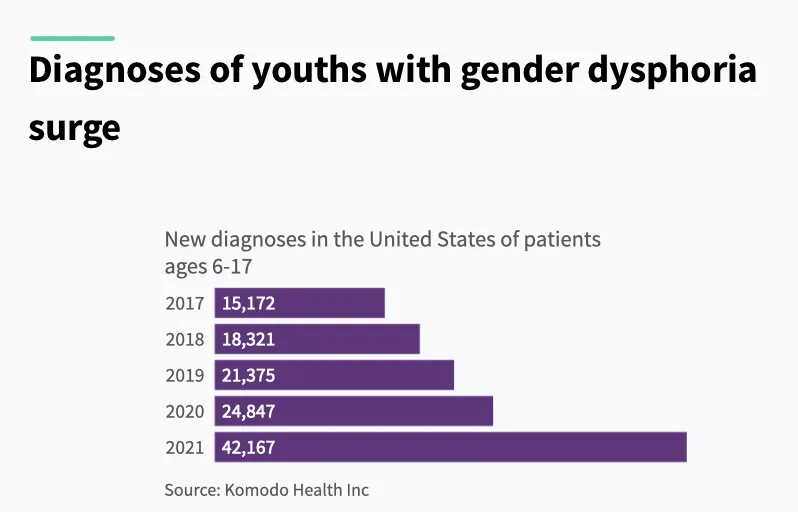
In the US alone, diagnoses among youth aged 6 to 17 nearly tripled—from around 15,000 in 2017 to over 42,000 by 2021—signalling a seismic shift not only in culture but in clinical practice.
Children diagnosed with gender dysphoria—a condition defined by distress related to one’s biological sex or associated gender roles—are increasingly being offered powerful medical interventions.
These include puberty blockers, cross-sex hormones, and, in some cases, irreversible surgeries such as mastectomy, vaginoplasty, or phalloplasty.
An umbrella review from the US Department of Health and Human Services (HHS) states that “thousands of American children and adolescents have received these interventions,” despite a lack of solid scientific footing.
While advocates often claim the treatments are “medically necessary” and “lifesaving,” the report concludes “the overall quality of evidence concerning the effects of any intervention on psychological outcomes, quality of life, regret, or long-term health, is very low.”
It also cautions that evidence of harm is sparse—not necessarily because harms are rare, but due to limited long-term data, weak tracking, and publication bias.
This 409-page report delivers a scathing review of the assumptions, ethics, and clinical practices driving gender-affirming care in the US.
An Inversion of Medical Ethics
At the heart of the HHS critique is a reversal of medical norms.
“In many areas of medicine, treatments are first established as safe and effective in adults before being extended to paediatric populations,” the report explains. “In this case, however, the opposite occurred.”
Despite inconclusive outcomes in adults, these interventions were rolled out for children—without rigorous data, and with little regard for long-term, often irreversible consequences.
These include infertility, sexual dysfunction, impaired bone development, elevated cardiovascular risk, and psychiatric complications.
“The physical consequences are often irreversible,” the report warns.
Puberty blockers, frequently marketed as a reversible ‘pause,’ actually interrupt bone mineralisation at a critical growth stage—raising the risk of stunted skeletal growth and early-onset osteoporosis.
When followed by cross-sex hormones, as is common, the harms multiply. Known risks include metabolic disruption, blood clots, sterility, and permanent loss of sexual function.
Yet many clinics operate under a “child-led care” model, where a minor’s self-declared “embodiment goals” dictate treatment.
The report notes that some leading clinics conduct assessments “in a single session lasting two hours,” often with no robust psychological evaluation.
Consent and Capacity
This raises a critical question: Are children capable of consenting to life-altering medical interventions?
According to the HHS, informed consent means more than simple agreement—it requires a deep understanding of risks, alternatives, and long-term impact.
And by definition, children lack full legal and developmental capacity for medical decision-making.
“When medical interventions pose unnecessary, disproportionate risks of harm, healthcare providers should refuse to offer them even when they are preferred, requested, or demanded by patients,” the report states.
Supportive parents cannot shield clinicians from ethical responsibility. Many children who present for transition also have autism, trauma histories, depression, or anxiety—all of which can impair decision-making.
Yet clinicians frequently misread a child’s desire to transition as evidence of capacity.
The report warns that the current affirmation model “undermines the possibility of genuinely informed consent” and that the “true rate of regret is not known.”
This becomes especially urgent when the outcomes—sterility, bone loss, and sexual dysfunction—are permanent. Can a 13-year-old grasp what it means to forgo biological parenthood?
As the report suggests, the system has failed to distinguish between a young person’s wish to transition and their developmental ability to understand what that means long term.
A Moral Failure
The problem is not only medical—it’s moral.
The HHS accuses the medical establishment of abandoning its core duty: to protect vulnerable patients. Ideology and activism, it argues, have taken precedence over evidence and caution.
“The evidence for benefit of paediatric medical transition is very uncertain, while the evidence for harm is less uncertain,” it states.
Among the most disturbing trends highlighted in the report is the sidelining of mental health support.
Research suggests that most cases of paediatric gender dysphoria resolve without intervention. Yet clinicians continue to proceed with irreversible treatments.
“Medical professionals have no way to know which patients may continue to experience gender dysphoria and which will come to terms with their bodies,” the report explains.
The Illusion of Consensus
The report also takes aim at the idea that gender-affirming care enjoys universal professional backing. It reveals that many official endorsements come from small, ideologically driven committees within larger organisations.
“There is evidence that some medical and mental health associations have suppressed dissent and stifled debate about this issue among their members,” it warns.
Several whistleblowers have spoken out—often at considerable personal risk.
Jamie Reed, a former case manager at the Washington University Transgender Center, alleged that children were being rushed into medical transition without adequate psychological screening. Her testimony led to a state investigation and Senate hearing.
Clinical psychologist Erica Anderson, a transgender woman and former president of the US Professional Association for Transgender Health, has repeatedly raised concerns about the haste with which children are put on medical pathways.
Dr Eithan Haim, a surgeon in Texas, is now facing prosecution after revealing details about paediatric gender surgeries at a children’s hospital.
Rather than sparking debate, these whistleblowers have faced vilification, career damage, and in some cases legal consequences. The HHS suggests this culture of fear has stifled the scientific inquiry necessary for sound medicine.
Psychotherapy as an Alternative
Instead of defaulting to hormones or surgery, the report urges a return to psychotherapy. Gender-related distress, it notes, often overlaps with broader psychological challenges that can be addressed non-invasively.
“There is no evidence that pediatric medical transition reduces the incidence of suicide, which remains, fortunately, very low,” the report finds.
Psychotherapy carries no documented harms and offers space for resolution and support. The HHS calls for greater investment in “psychotherapeutic management” as a safer and more ethical approach.
Restoring Scientific Integrity
Commissioned under President Trump’s Executive Order Defending Children’s Innocence by Ending Ideological Medical Interventions, the report responds to growing alarm over the medicalisation of minors.
Trump’s Executive Order directed federal agencies to evaluate practices to help “minors with gender dysphoria, rapid-onset gender dysphoria, or other identity-based confusion, or who otherwise seek chemical or surgical mutilation.”
It explicitly criticised “junk science” promoted by groups such as the World Professional Association for Transgender Health (WPATH), calling for a return to evidence-based standards and scientific discipline.
Rather than imposing new mandates, the HHS report focuses on delivering “the most accurate and current information available” to clinicians, families, and policymakers—urging caution and restraint.
“Our duty is to protect our nation’s children—not expose them to unproven and irreversible medical interventions,” said NIH Director Dr Jay Bhattacharya. “We must follow the gold standard of science, not activist agendas.”
Reform Already Underway
The HHS report lands amid a wave of legal reforms.
As of this year, 27 states have passed laws restricting or banning gender-affirming care for minors. These range from full bans on hormones and surgery to tighter consent requirements.
Nineteen of those laws were passed in 2023 alone, according to the Kaiser Family Foundation.
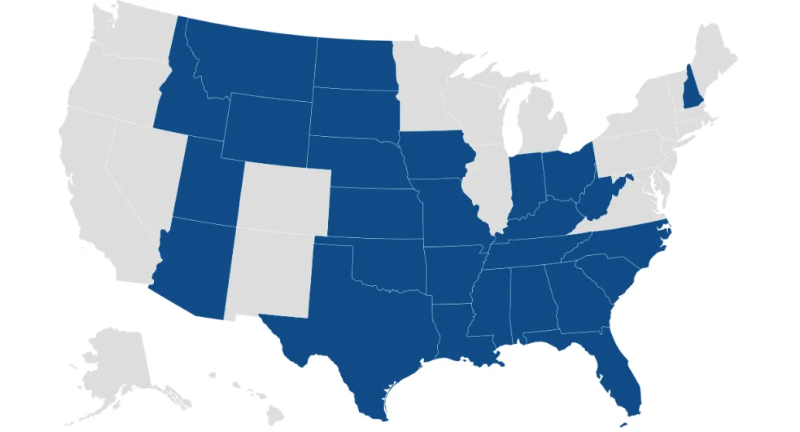
Over half of states have enacted laws/policies limiting youth access to gender affirming care Though many face court challenges, the trend reflects mounting public concern over the medicalisation of gender-distressed youth. The HHS findings are expected to accelerate further scrutiny and legislative action.
Global Shifts
The HHS review is part of a broader international movement to re-examine paediatric gender medicine.
In 2024, the UK’s Cass Review, led by paediatrician Dr Hilary Cass, delivered a landmark critique of NHS gender services. Cass concluded that the model had been adopted prematurely “based on a single Dutch study,” and lacked sufficient evidence.
In response, the UK banned the routine use of puberty blockers and began closing the Tavistock gender clinic, replacing it with regional centres focused on holistic mental health care.
In Australia, the Queensland government took similar steps earlier this year, pausing all prescriptions of puberty blockers and cross-sex hormones for minors pending further review.
The move followed the suspension of Dr Jillian Spencer, a senior psychiatrist, from her clinical duties at Queensland Children’s Hospital after she raised concerns about the gender care protocols being used.
Her case has since become a focal point in Australia’s national debate on youth gender medicine.
A Reckoning
The HHS report is more than a policy review—it is a warning.
It reveals that thousands of children—many struggling with underlying psychological issues—have been placed on a path of irreversible medicalisation without the basic safeguards expected in any other area of healthcare.
The report concludes that gender medicine has been practised backwards – treatments were introduced first, and only later did the search for evidence begin.
It calls for a course correction—one that puts evidence before ideology, and ethics above political expediency.
Whether institutions will act on its findings remains to be seen. But for families searching for answers, the report may finally provide the long-overdue clarity that has been obscured by years of activism and politics.
Republished from the author’s Substack
================================================================
Author
Maryanne Demasi, 2023 Brownstone Fellow, is an investigative medical reporter with a PhD in rheumatology, who writes for online media and top tiered medical journals. For over a decade, she produced TV documentaries for the Australian Broadcasting Corporation (ABC) and has worked as a speechwriter and political advisor for the South Australian Science Minister.
Gender twisting mutilation.
i foresee a massive wave of class action lawsuits against parents, institutions, and individuals as the children who have been mutilated start to grow up and realize that they’ve had their lives permanently wrecked ... that will end this wanton destruction, but until such a wave happens, the wanton destruction will continue ...
“Any idea when parents and teachers will realize kids should
identify with Felix the Cat?”
has come and gone: some time back, schools were allowing children who identified as cats to relieve themselves in litter boxes ... i THINK that nonsense has ended ...
“When these 46,000++ children grow to be adults with life ruining injuries, I pray they take every action possible to financially ruin the lives of those adults who destroyed them.”
exactly: massive class action lawsuits ... which is the only thing that will end this insane destruction of children’s lives ...
I wonder where these kids got the idea they weren’t the correct gender?
$$$$$$ are at stake. And that is the main reason providers see “gender affirming care” as a positive.
‘Gender Affirming Care’. Sure sounds better than ‘Delusion Pandering Mutilation’ which is the same thing.
At all.
And reopen the ones we closed down.
Same folks who convinced 24.5% of teens in 2024 they are Gay/Bi/Queer/Etc, vs. 1% in 1970
No more gender-bending medical interventions!
Make children’s hospitals healthy again!
There are two conditions where puberty blockers are a corrective protocol; congenital adrenal hyperplasia and non-classic congenital adrenal hyperplasia. In both instances, it helps mitigate the negative effects of these incurable endocrine disorders.
In the case of Klinefelters (XXY chromosomes), young boys need additional testosterone to offset the effects of the additional female chromosomes on their puberty development.
In the case of Turners Sydrome (X or X/partial X), young girls need hormones boosts to ensure proper sexual development.
In the case of Swyers, it’s more complicated. These youngsters have XY chromosomes and a vagina, typically with undescended testes. They are incomplete males but present at birth as female.
These and several other extremely rare endocrine disorders can alter brain chemicals and cause gender dysphoria. Not everyone who has one of these conditions will be dysphoric and those that do will not always remain dysphoric once puberty ends.
Dr. Kenneth Zucker was regarded for decades as the world’s leading expert on this issue. His approach included genetic testing, an endocrinologist, a psychiatrist, a therapist, and the child’s regular doctor, with the focus on making the child comfortable with their body instead of altering it.
Radical trans activists lied about him, forced him out of his clinic, kicked him off boards, and changed the protocols. That was when the “trans” movement exploded.
It is statistically impossible for all these people to be trans. I know; my kid is one of the people with NCCAH and it has been a painful, isolating condition they would not wish on anyone.
If there is no underlying medical condition, then it’s mental and surgery won’t cure it.
Moreover, actual science clearly shows there is never a need to transition children. The only surgery should be corrective, in the case of intersexed children (born with both sets of parts).
Still conflicted re. the abortion issue? Please watch this 6 minute video explaining why abortion is an act of cultural & national SUICIDE! DOES AMERICA ALSO HAVE A DEATH WISH? MUSLIM CONQUEST BY OUT-BREEDING THE WEST! It's happening as you read this. 6 minute video explains:
https://www.youtube.com/watch?v=erSH_0dKAks
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.