
Posted on 01/04/2022 8:57:37 PM PST by MinorityRepublican
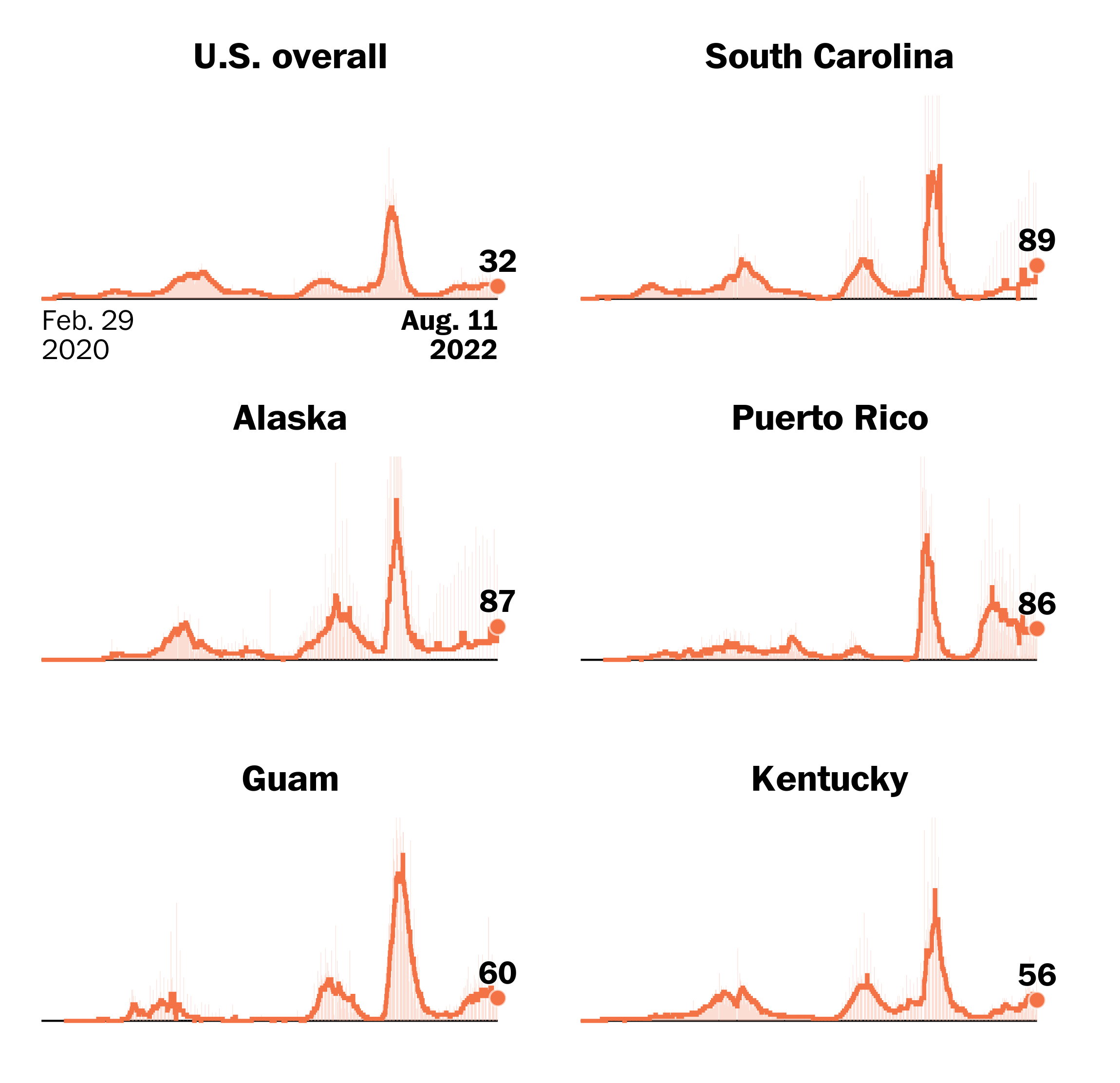
Places with highest daily reported cases per capita
Seven-day average of daily new reported cases per 100,000 residents

https://www.wtsp.com/article/news/health/coronavirus/coronavirus-numbers/florida-hospitalizations-covid-cases/67-dfc43d8b-b960-456c-8fcb-7b6e477c2955
So far we seem to be following the SA curve vice the UK. I’m sure there will be regional hospital surges (and they will be hyped in the headlines), but hopefully the trend of very low mortality continues.
In Indonesia, with a population of 273 millions, we are averaging 8 C19 deaths per day since October. Is there something in the water in America?
Younger and healthier population in Indonesia.
I have traveled to 40+ countries on 4 continents.
I never saw so many fat people anywhere as I see here in USA. Covid likes fat people.
If that were the case then covid would hit hard with males wearing speedos on European beaches. /s
We blame all deaths on covid if tested positive, so it artificially raises the number
Merck’s oral COVID-19 pill molnupiravir (Lagevrio) is just the kind of toxic 'make-it-worse' faux treatment we've learned to expect the FDA/CDC/NIH/Fauci machinery to foist upon the public.
Placebo group had fewer hospitalizations than Molnupiravir. That must have been what 'sealed-the-deal' for the medical coup machinery to push it out the hatch. Article by Dr. Joseph Mercola.
Merck’s New Covid Pill Is a Disaster – Freedom First Network
| In the General/Chat forum, on a thread titled Frontline Doctor Highlights His Preferred COVID-19 Treatments: 4,000 Patients Treated with only Five Ending Up in Hospital, None Dead, silverleaf wrote: |
Those pills..... are both awful Report by Dr Mercola Meanwhile IVM is still being derided as untested and unproven? |
USA = exceptionally mobile population with plenty of co-morbidities and very little mitigation outside of a modest rate of vaccinations.
AND... Indonesia DID hit over 2k fatalities a day back in late July and early August 2021. But, you don’t have virus weather like we do, in Oct. to March, to reinvigorate the wave.
FWIW, the best vid I’ve seen on effective and safe use of N95 masks was from Indonesia, featuring a lovely Indonesian nurse. Our CDC is not smart enough to provide such education!
Indonesia’s COVID CFR hit around 3.5% a few months ago, with deaths spiking over 2k / day. The real difference is that their wave of cases passed, and ours persisted.
“It’s 2022 and the CDC has terminated the use of the PCR, which it concedes does not identify Covid.”
Of course that’s not true, but it’s not surprising that you keep repeating it. Your indifference to truth is becoming legendary.
The CDC announced back on July 21 2020 that they were going to replace the then current PCR test with an improved model that can do more. The old test worked just fine for identifying the Covid virus. They are simply carrying out the planned replacement. You know this, you’ve had the links posted to you.
And here it is once again:
After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives.
Visit the FDA website for a list of authorized COVID-19 diagnostic methods. For a summary of the performance of FDA-authorized molecular methods with an FDA reference panel, visit this page.
In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. Such assays can facilitate continued testing for both influenza and SARS-CoV-2 and can save both time and resources as we head into influenza season. Laboratories and testing sites should validate and verify their selected assay within their facility before beginning clinical testing.
| In the General/Chat forum, on a thread titled WORLDOMETER COVID-19 Deaths in USA 1/4/2022: 1,847 with 567,696 new cases, Pelham wrote: |
“It’s 2022 and the CDC has terminated the use of the PCR, which it concedes does not identify Covid.” Of course that’s not true, but it’s not surprising that you keep repeating it. Your indifference to truth is becoming legendary. The CDC announced back on July 21 2020 that they were going to replace the then current PCR test with an improved model that can do more. The old test worked just fine for identifying the Covid virus. They are simply carrying out the planned replacement. You know this, you’ve had the links posted to you. And here it is once again: After December 31, 2021, CDC will withdraw the request to the U.S. Food and Drug Administration (FDA) for Emergency Use Authorization (EUA) of the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel, the assay first introduced in February 2020 for detection of SARS-CoV-2 only. CDC is providing this advance notice for clinical laboratories to have adequate time to select and implement one of the many FDA-authorized alternatives. Visit the FDA website for a list of authorized COVID-19 diagnostic methods. For a summary of the performance of FDA-authorized molecular methods with an FDA reference panel, visit this page. In preparation for this change, CDC recommends clinical laboratories and testing sites that have been using the CDC 2019-nCoV RT-PCR assay select and begin their transition to another FDA-authorized COVID-19 test. CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza viruses. Such assays can facilitate continued testing for both influenza and SARS-CoV-2 and can save both time and resources as we head into influenza season. Laboratories and testing sites should validate and verify their selected assay within their facility before beginning clinical testing. |
The PCR has falsely identified Coca Cola, Orange Juice, Kiwi fruit and 'Spanish Water' as Covid positive. I've posted over and over and over again that the inventor of the PCR explains why it simply cannot diagnose an illness.
Even Fauci and CDC are now publicly admitting you can remain positive months after you are no longer ill, but you still wanna play that game, eh?
10/26/2021, 5:48:25 PM · by ransomnote · 28 replies
FDA document admits “covid” PCR test was developed without isolated covid samples for test calibration, effectively admitting it’s testing something else
fos-sa.org ^ | August 2, 2021 | Naomi Wolf
One FAKE PCR ‘Test’ to rule us all. How the CDC/FDA/NIH and World Health Organization made themselves gods.
8/25/2021 | vanity
12/8/2021, 6:19:23 PM · by Fractal Trader · 55 replies
CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel [inludes my remarks, images from document, and the download link for the document]
fda.gov ^ | 07/21/2021 | CDC/DDID/NCIRD/ Division of Viral Diseases
Lies, Damned Lies and Health Statistics – the Deadly Danger of False Positives
lockdownsceptics.org ^ | September 20, 2020 | Dr Michael Yeadon
PLAGUE OF FEAR 2020 - Part 7 - THE NAIL IN COVID'S COFFIN
hive.blog ^ | Jan 31, 2020 | Steve Falconer, francesleader
Indonesia, like most of Asia, has not yet had their Omicron wave.
It won’t be long, until you do.
Case, case, cluster, cluster, BOOM!
The boom seems to shoot up for about 3-4 weeks, to the highest new daily case rates of the pandemic, then drop back down. It is not as bad with hospitalizations and deaths as the earlier major strains.
By the time Indonesia is booming, there will have been a of other examples to study (South Africa, USA, Europe), so it will be more understood and predictable.
Some States/Localities are already showing a leveling off for a few days (Florida, DC, Maryland, New Jersey).
It may just be hitting the test capacity limit, but I am looking for the places that started earlier, to start cresting earlier.
I am still hoping that the surge in hospitalizations is significantly because of people with mild or no symptoms who happen to test positive when going to hospital for other reasons. The high test positivity rate would seem to indicate that a wider cross section of the public is now infected.
All BS all the time. The numbers are pure lies.
For the Covid Cultists and Fauci Fanatics it’s like Christmas every time you post these.
Shut down the MSM and social media and covid-19 wouldn’t exist.
The tests results are severely flawed, mask don’t work and never have for this type of airborne disease, the gene therapy doesn’t work and are causing serious illnessesbut facts are just not science.
https://coronavirus.jhu.edu/
Data as of 5 January 2022
( 830,375 “U.S. Deaths” / 331,002,651 ) x 100 = 0.251 %
Over TWO years time frame, one quarter of one percent “officially” dead from the case-demic.
Given that the tally now extends a full two years, simple averaging by year brings the “event” down to half the official deaths tally PER YEAR.
And then the percent dead in the case-demic population also drops by half, to little more than twelve one-hundreths of one percent.
Reporting continual “cases” as if each case represents a significant illness, and each illness leads possibly to death is foolish. As the post observes, this day “with 567,696 new cases” are tallied, which is more than a one-year tally of official deaths.
We are enjoying a case-demic, seen by the reporting itself.
But it is marvelous MARKETING.
First, the government and its allies pay for most of the marketing, while the mRNA manufacturers — already shielded from product liability law suits — are seeing the marketing of their products done for them.
Second, the enthusiasts for such reporting pass the marketing message on. Amplification of the almost cost-free to the manufacturers' marketing message is done, also cost-free.
Third, those skeptical of the BS are rebuffed by those who BELIEVE, and present data as if it tells what it does not tell.
“...with 567,696 new cases” is a remarkable number, given two years’ of “official” death is 830,375 as of today.
Someone could be misled into thinking the “numbers” were foretelling massive new numbers of COVID-19 deaths. The numbers simply do not say that.
Why would there be a surge in hospitalizations, now, “for other reasons”?
Granted that docs and nurses in my area (Mid-South USA) are reporting lots of parallel infectious disease cases. Not so much flu, as a whole variety of other stuff.
My guess though, is that although Omicron is dominating, Delta is still “out there” doing well in “cold and flu season”, and many people are not taking any precautions at all.
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.