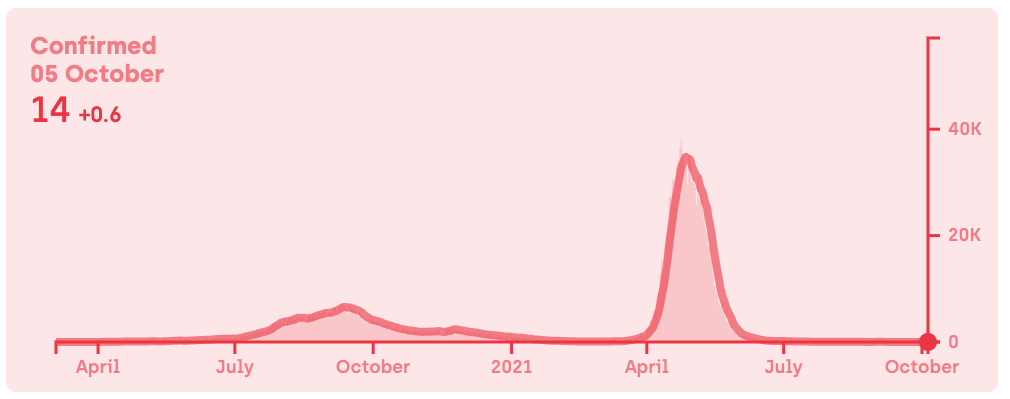
Figure 1. Daily number of confirmed COVID-19 cases in Uttar Pradesh between 4 March 2020 and 5 October 2021. Daily new confirmed cases are presented as the rolling 7-day average. Data and image from covid19india.org.
Posted on 01/01/2022 9:14:39 AM PST by SeekAndFind
FULL CLAIM:
"The most populated state in India just declared they are officially COVID-19 free after promoting widespread use of the safe proven medicine"
In mid-September 2021, a similar claim that the Indian state of Uttar Pradesh had become COVID-19 free, proving the effectiveness of [the] ‘deworming drug’ Ivermectin” spread on outlets, including One America News Network (OAN), The True Defender, and Gateway Pundit. Versions of the claim received more than 100,000 interactions on social media platforms like Facebook, Instagram, Reddit, and Twitter, according to the social media analytics tool CrowdTangle.
The government of Uttar Pradesh started recommending the use of ivermectin to prevent and treat mild COVID-19 patients in August 2020. By comparing the epidemiological data in Uttar Pradesh with other Indian states and the U.S., these outlets suggested that ivermectin is more effective than COVID-19 vaccines to control the pandemic. However, no scientific evidence supports this claim, as we will explain below.
According to data from covid19india.org, a project spearheaded by volunteers dedicated to documenting COVID-19 statistics using multiple official sources, Uttar Pradesh suffered two COVID-19 waves peaking around mid-September 2020 and end-April 2021 (Figure 1).
Figure 1. Daily number of confirmed COVID-19 cases in Uttar Pradesh between 4 March 2020 and 5 October 2021. Daily new confirmed cases are presented as the rolling 7-day average. Data and image from covid19india.org.
In September 2021, the regional government announced a 99% decline in the number of cases that some linked to ivermectin recommendations. However, Uttar Pradesh isn’t “COVID-19 free”, as some outlets claimed (see examples here and here). Although the state reported only 147 active COVID-19 cases as of 7 October 2021, only 37 of its 75 districts have been declared free of COVID-19.
Furthermore, the difference between the number of confirmed COVID-19 cases and the percentage of the population with antibodies against SARS-CoV-2 (seroprevalence) indicates that India is largely undercounting SARS-CoV-2 infections. This underreporting is unevenly distributed among regions, making it difficult to compare the epidemiological situation in different states.
For example, Kerala currently accounts for about half of the new COVID-19 cases in India. OAN and Gateway Pundit claimed that this was proof that this state, which they described as “over-dependent on vaccines and less dependent on Ivermectin”, failed to control COVID-19 cases. However, estimates from July 2021 based on seroprevalence studies indicated that, at that time, Kerala had a far more effective testing strategy than Uttar Pradesh. While Kerala detected one COVID-19 case every six, Uttar Pradesh only detected one case every 100. This means that Kerala doesn’t necessarily have more COVID-19 cases than Uttar Pradesh, but rather might have detected a higher proportion of them.
Simply because two events happened at the same time doesn’t necessarily mean that one caused the other. In other words, correlation alone doesn’t imply causation. Instead, this correlation can be coincidental or the result of a third “confounding factor” that affects the other two events. For instance, the fact that drownings increase at the same time that ice cream consumption doesn’t mean that eating ice cream causes drowning. What happens is that both events are more frequent when the weather is hot, which is the confounding factor.
Likewise, the ivermectin recommendation didn’t necessarily cause the current drop in COVID-19 cases in Uttar Pradesh, which can be due to other factors. In an article for The Conversation, epidemiologist Rajib Dasgupta explained that the sharp decline in COVID-19 cases in June 2021 might be due to the high proportion of previously infected individuals, combined with COVID-19 vaccination and increased testing.
Indeed, the fourth nationwide seroprevalence study conducted by the Indian Council of Medical Research (ICMR) in June and July 2021 showed that 67.6% of the population over the age of six had antibodies against SARS-CoV-2 as a result of either vaccination or previous infection. This figure is much higher than in the previous three national serosurveys (0.7% in May-June 2020, 7.1% in August-September 2020, and 24.1% in December 2020-January 2021)[1].
While previous infections account for a proportion of this high seropositivity rate, COVID-19 vaccination also plays an important role. As of 7 October 2021, almost 40% of the Indian population received at least one dose of the COVID-19 vaccine, and 18% is fully vaccinated, according to Our World in Data. Based on data collected between April and August 2021, Indian public health experts found that a single dose of the COVID-19 vaccine is “96.6 percent effective in preventing death”.
The fact that many people have antibodies against the virus means that a large proportion of the population is protected from disease to a certain extent, reducing the chances of new infections happening. In late July 2021, an article in the Hindustan Times reported that Uttar Pradesh was one of the states with the highest seropositivity rate (71%).
Interestingly, Kerala had the lowest seropositivity rate (44.4%). Notably, at that time, 35% of its population had received at least one dose of the COVID-19 vaccine and almost 20% were fully vaccinated. These statistics taken together suggest that the seropositivity was mainly the result of vaccination, not infection. This suggests that Kerala was more effective at slowing the spread of the virus in the early stages of the pandemic than in the rest of the country. In a New York Times article published in May 2021, health experts explained that this result was due to a combination of high investment in healthcare and rigorous testing and contact tracing strategies from the beginning of the pandemic.
Finally, OAN claimed that ivermectin allowed Uttar Pradesh to control COVID-19 “without the need of lockdowns” and other restrictions. This is false. The administration of Uttar Pradesh did implement restrictions to curb the spread of the virus, including a complete lockdown on 30 April 2021. The lockdown was extended several times across May 2021, followed by night and weekend restrictions until September 2021.
Uttar Pradesh’s government did release guidelines recommending ivermectin to treat mild COVID-19 patients in August 2020. However, this recommendation isn’t on its own proof that the Uttar Pradesh population used the drug more than populations in other states.
Furthermore, ivermectin has been promoted throughout the country at some point during the pandemic, particularly in some states such as Goa. And during the second COVID-19 surge, India’s Ministry of Health & Family Welfare included ivermectin as a possible treatment for patients with mild COVID-19. On 17 May 2021, the Indian Council of Medical Research (ICMR) followed suit, although it acknowledged the low quality of evidence supporting ivermectin use in COVID-19 patients. But like in the case of Uttar Pradesh, we don’t know whether these recommendations translated into greater ivermectin use among the population.
OAN’s claim that ivermectin is one of the “safest, most effective medicines in the world” is also misleading. This status only applies to the concentrations and conditions recommended for treating parasitic infections, not as an antiviral in COVID-19 patients.
Public health agencies, including the World Health Organization and the U.S. Food and Drug Administration, warn about the lack of clear evidence supporting claims about ivermectin’s effectiveness in reducing disease severity, hospitalization, or mortality in COVID-19 patients. Gideon Meyerowitz-Katz, an epidemiologist at the University of Wollongong in Australia, explained in his blog that most of the studies so far evaluating the effectiveness of ivermectin against COVID-19 have important methodological limitations, including small sample sizes and a small number of events.
Notably, one of the studies that contributed to positive assessments of ivermectin as a COVID-19 treatment was withdrawn in July 2021 over ethical concerns. As Health Feedback explained on numerous occasions (here, here, here, and here), more reliable studies didn’t find a benefit of the drug in COVID-19 patients. In a July 2021 Cochrane review of 14 previous studies, the authors concluded, “we are uncertain whether ivermectin reduces or increases mortality compared to no treatment”[2]. Given the lack of evidence supporting ivermectin’s use, the ICMR removed this drug from the September 2021 update of its COVID-19 treatment guidelines.
The claim that Uttar Pradesh is now COVID-19 free due to the use of ivermectin is inaccurate and unsupported by scientific evidence. Uttar Pradesh isn’t entirely free of COVID-19, and comparisons with other states are challenging due to differences in testing capacity. Furthermore, many factors other than ivermectin use could have influenced the course of the second COVID-19 wave in Uttar Pradesh, including restrictions and immunity from previous infection and vaccination.
In addition, the quality of evidence supporting ivermectin use in COVID-19 patients is very low. For this reason, public health authorities don’t recommend the use of ivermectin for preventing or treating COVID-19 outside of clinical trials. Given all these uncertainties, we can’t determine whether ivermectin played any role at all in the decline of COVID-19 cases in Uttar Pradesh.
If this is the one, it will not complete until May 31, 2022:
https://clinicaltrials.gov/ct2/show/results/NCT04703205
So, looks like we’ll have to keep checking on it.
Looking at that NIH article its a study of other researcher's studies.
https://www.ncbi.nlm.nih.gov/pmc/articles/instance/8394824/bin/ciab591_fig1.jpg

What I do see is that out of 256 records regarding Ivermectin they kept 10 and excluded 246 of the records. How much Ivermectin was given? Did they have an effective dose or were the patients given amounts below an effective level? How long did they receive it?
Because of these questions I would probably try to find an actual study rather than an extrapolation from other peoples works. You can select your studies to support your expected conclusion and I do not think either of us is inclined to review the other 246 studies for content!
https://www.scientificamerican.com/article/trial-sans-error-how-pharma-funded-research-cherry-picks-positive-results/
By Ben Goldacre on February 13, 2013
I think there is actually a lot of pressure to NOT find Ivermectin effective! See;
https://www.worldtribune.com/researcher-andrew-hills-conflict-a-40-million-gates-foundation-grant-vs-a-half-million-human-lives/
"On Jan. 6 of 2021, Hill testified enthusiastically before the NIH COVID-19 Treatment Guidlelines Panel in support of ivermectin’s use. Within a month, however, Hill found himself in what he describes as a “tricky situation.” Under pressure from his funding sponsors, Hill then published an unfavorable study. Ironically, he used the same sources as in the original study. Only the conclusions had changed.
Shortly before he published, Dr. Tess Lawrie, Director of the Evidence-based Medicine Consultancy in Bath, England, and one of the world’s leading medical research analysts, contacted Hill via Zoom and recorded the call (transcript below). Lawrie had learned of his new position and reached out to try to rectify the situation.
In a remarkable exchange, a transcript of which appears on pages 137 – 143 in Kennedy’s book, Hill admitted his manipulated study would likely delay the uptake of ivermectin in the UK and United States, but said he hoped his doing so would only set the lifesaving drug’s acceptance back by about “six weeks,” after which he was willing to give his support for its use"
Yes, that’s what a metal study is. A review and meta-analysis of published studies. Studies may be excluded for a number of reasons (size, mouse study, in vitro, methods). Two reasons given for excluding on the second sort were “no control group” and “sole outcome of no interest”.
If you want to see actual, individual studies, you can find them here:
https://pubmed.ncbi.nlm.nih.gov/?term=covid+ivermectin
I agree, no way would I be willing to go through all 243 studies!
My personal opinion: Ivermectin may be of some small benefit. After we got MABs, why bother with it? But now that the Biden administration (whoever they are) is yanking MABs ... gulp.
Actually, by going to the search link I posted, you can see several entries in the first half of the first page which should not be included. A proposal for a clinical trial, a letter to the editor, a proposal for study based on in vitro, etc. Not actual human clinical trials or even close. I would not be surprised to find 243 like that on PubMed!
Thanks! I am not going to look further tonight. I recollect that when I see Ivermectin mentioned it is generally as part of a protocol. No, Regneron is no longer for the proles and peons apparently!
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.