Skip to comments.
NY TIMES: Up to 90% Who’ve Tested COVID-Positive Wrongly Diagnosed! TRUTH: A Whole Lot Worse! (Parts 1, 2 and 3)
Red State ^
| 09/03/2020
| Michael Thau
Posted on 09/03/2020 12:30:51 PM PDT by SeekAndFind
PART 1
“The man who reads nothing at all is better educated than the man who reads nothing but newspapers.”
―
The New York Times just reported something incredible.
You know those standard PCR tests for the COVID-19 virus that everybody in America has been rushing out to get? Well, according to the Times, they’re “diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus” and “are not likely to be contagious.”
In fact, when they looked at three sets of testing data from Massachusetts, New York, and Nevada, the Times says that, because of faulty procedures used at every single testing site in the country, “up to 90 percent of people testing positive carried barely any virus” at all.
The experts they talked to were astonished that such cases are even getting classified as infections.
Not surprising since, as we’ll see, in the first of many curious understatements about how bad the scandal they’re reporting on really is, the research the Times cites actually suggests that those bogus positive tests they discovered were given to people carrying no virus whatsoever, not just insignificant amounts, as they report. And they’re upper bound of 90% for bogus positives is likely too low as well.
But, since they do admit that defective methods which are standard operating procedure literally everywhere inflated the number of positive tests by a factor of ten in one random sample, this would be big news even were it no worse than the Times is letting on.
Over 85 million PCR tests were given in the U.S. since dreading COVID-19 replaced baseball as our national pastime. At around $15o a pop, that’s almost $13 billion that, if the New York Times is right, was flushed down the toilet on a test that’s essentially worthless.
Not to mention all the wasted hours and inconvenience suffered.
The massive fraud perpetrated on the American people – who were led to believe that PCR testing represents the “gold standard” for detecting COVID-19 infections – must be one of the biggest scams in history.
Apart from the squandered money, think of all the anxiety suffered by the over 7 million Americans who got back a positive result. Yet, even according to the Times, most of them – and maybe even the vast majority – likely had only traces of the virus too minute and harmless to classify as an infection.
Philadelphia’s Temple University just canceled all in-person classes for every single one of its 40,000 students for at least two weeks because 103 of them tested positive for COVID-19. The Times report appears to show that all that uproar and disruption – which has been breaking out incessantly all across America for months now – had no justification.
Last week I reported that the enormous “second wave” of COVID-19 infections America supposedly suffered in July never really happened. That steep rise in the daily number of positive tests we heard so much about was caused by a massive increase in the number of people being tested every day that we didn’t.
The Times report, however, makes the increase in absolute case numbers itself garbage. According to the experts they consulted, procedures universally applied caused 90% of the positive diagnoses in one randomly selected set of tests to be bogus.
So you’d think the New York Times would be trumpeting their findings as an earth-shattering piece of investigative reporting and maybe even dusting off a place on the shelf for a Pulitzer Prize.
But this is another area where the Times exhibits a strange reluctance to run with the implications of their own report.
That eye-popping stat that “up to 90 percent of people testing positive carried barely any virus” isn’t even featured in the headline. Instead, the Times went with one that couldn’t possibly have downplayed their astonishing discovery more:
Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
Moreover, not once does the Times even mention all the money and time wasted or the havoc unleashed because Americans were encouraged to falsely believe that a test they’re now reporting is complete garbage was “the gold standard.”
Their story is written from the same “destroy the village to save it” perspective that’s guided our response to COVID-19 since the early days in March, when it suddenly became the idée fixe dominating every second of our lives.
Slowing down COVID’s spread by any means necessary is presented as the only thing that matters. Not inflicting collateral hardship, misery, and death on the American people doesn’t even register as a priority.
Nor, of course, does respecting our rights.
And the key to unlocking the mystery of why the New York Times is exposing a tiny part of an historically unprecedented scandal while making sure to keep the rest firmly out of sight lies in the perfect means COVID-19 has provided for convincing the American people to surrender their God-given right to liberty without even putting up a fight.
… Part 2 is up.
Same Red-time.
Same Red-channel.
PART 2
***
“Quantitative PCR is an oxymoron.”
Nobel Prize-winning inventor of PCR, Kary Mullis on why it can’t be used to test for viruses
***
In the previous entry, we learned about The New York Times’ shocking report that the standard PCR tests for COVID-19 everyone’s been rushing out to get are woefully unreliable.
The Times looked at three sets of PCR testing data from Massachusetts, New York, and Nevada and discovered that, because of faulty procedures used at every single testing site in the country, “up to 90 percent of people testing positive carried barely any virus” at all.
The experts they talked to were astonished that such cases are even getting classified as infections.
Yet, for some reason, the Times ran a weak-sauce headline completely downplaying their scandalous discovery: Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
But those eye-popping stats exposing the pervasive fraud propping up our regime of mass COVID-19 testing aren’t just absent from the headline. Readers don’t find out about the enormous percentage of faulty diagnoses the Times discovered until their article’s half over!
The opening paragraph briefly states what they found, but only in very general and decidedly less alarming terms:
Some of the nation’s leading public health experts are raising a new concern in the endless debate over coronavirus testing in the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus.
And it’s used as a means to immediately segue into a quite different topic, which the entire first half of the article – aka, the only part anyone’s likely to read – is devoted to:
But researchers say the solution is not to test less, or to skip testing people without symptoms, as recently suggested by the Centers for Disease Control and Prevention. Instead, new data underscore the need for more widespread use of rapid tests…
You may not have heard about those new CDC recommendations to stop testing people without symptoms about which the Times and their anointed experts aren’t thrilled. But their significance can’t possibly be overstated because of a crucial feature of any test that somehow never seems to come up in all the media articles pushing for mass COVID-19 testing: the rate of false positives.
Because any test for COVID-19 will produce a certain percentage of positive diagnoses for patients who don’t, in fact, have the virus, mass testing means that alarming numbers of new COVID-19 cases will keep getting reported every day no matter how few are actually occurring.
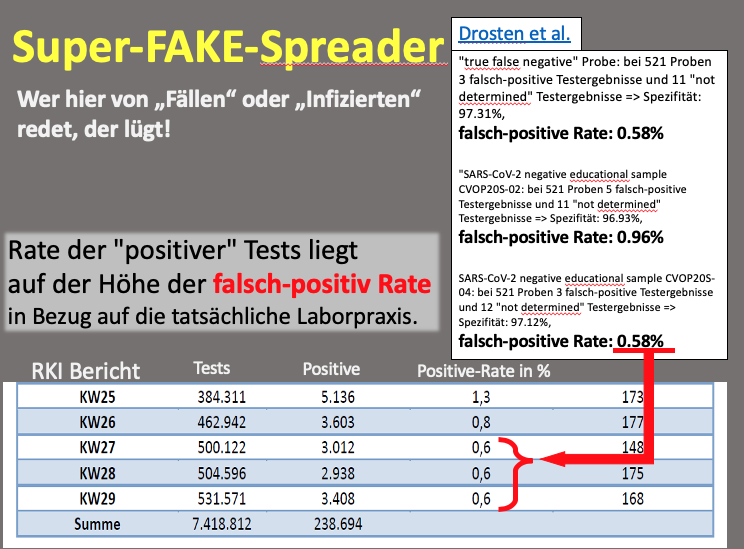
The FDA says that one test in use has a false positive rate of 3%. That means that testing a million people a day with it would still result in 30,000 positive diagnoses being reported each day even if the real number of new infections dropped all the way down to zero!
If everyone in America were tested daily as some have proposed, even a .5% false-positive rate would result in over a million and a half new cases being reported daily in the absence of any actual new infections.
The fact that any test is going to have a non-negligible rate of false positives makes mass COVID-19 testing a means for ensuring that a phony pandemic will persist forever even after the real one has run its course.
It may already be happening in Germany.
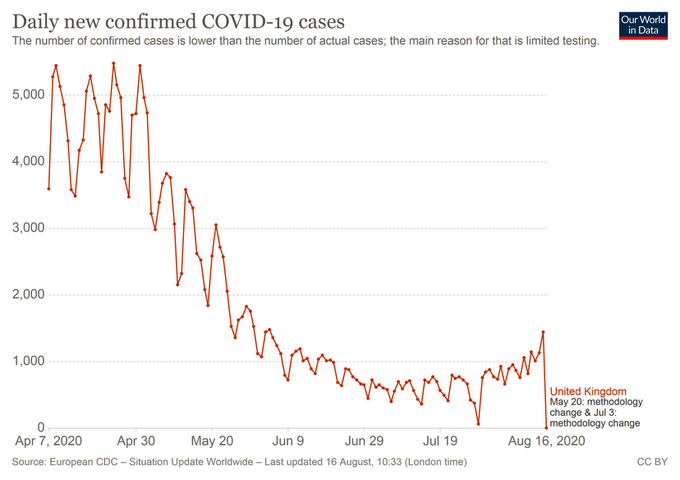
And in the UK as well.
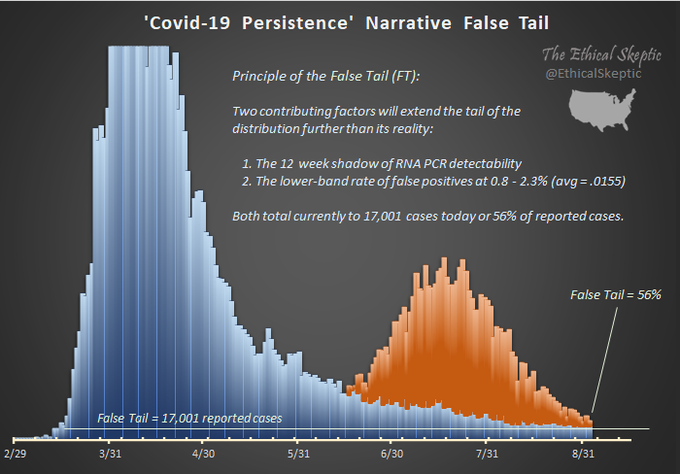
And we’re getting there in the U.S.
It’s important to understand, however, that the massive errors in PCR testing reported in that New York Times story are not, strictly speaking, false positives. They, instead, represent an additional much larger source of bogus COVID-19 diagnoses.
They don’t occur because the test found something that wasn’t there. They’re a product of the faulty criteria laboratories are using to determine when to label perfectly accurate test results positive.
The problem starts because what the PCR test is designed to find is NOT the COVID-19 virus.
That’s going to surprise a lot of people given what our own public health officials have been telling us:
- The CDC says that “A viral test checks samples to find out if you are currently infected with COVID-19.”
- According to the Department of Health, The University of Colorado, and a host of other sources many Americans rely on: “A positive PCR test means that the person being tested has an active COVID-19 infection.”
But these claims represent either deliberate deceptions or the grossest possible incompetence.
“PCR” stands for polymerase chain reaction, the biochemical process developed by a researcher named Kary Mullis in 1983 that the test uses.
Though it was important enough to earn Mullis a Nobel Prize, most are unaware that PCR wasn‘t designed to test for viruses at all.
Mullis invented it to synthesize genetic material for research purposes and, in fact, was strongly opposed to the way it wound up being used to test for the HIV virus.
Mullis’s process takes segments of DNA through a “cycle” that doubles the amount. That might not seem like a big deal, but it starts to add up pretty quickly.
If, for example, you ran a single segment of DNA through just 40 PCR cycles, you’d end up with 1 x 240 segments, which is over a trillion new copies.
Because viruses aren’t much more complicated than strands of DNA, it’s possible to use PCR to amplify any viral byproducts in a sample.
Most people probably think of viruses as microorganisms similar to bacteria. But they’re, in fact, much more primitive than bacteria and usually aren’t even classified as living things. They’re not composed of cells, nor do they create their own energy or grow.
Believe it or not, viruses can’t even reproduce on their own but, instead, have to trick their host organisms into doing all the work. In fact, performing that one trick is pretty much all there is to them.
Viruses are nothing more than small bits of genetic code surrounded by a shell that acts as a “Trojan horse.” Its shell allows a virus to invade the cells of living organisms. Once inside, the genetic code exits the shell, hijacking the cell’s functions to make it produce more copies of the virus.
The genetic material inside a virus’s shell can be either DNA or RNA. The COVID-19 virus contains the latter. Mullis’s process, however, works only on the former. So before it’s applied to test for COVID, another process is used to convert any RNA in the sample to DNA. Once that’s done, the sample is run through a number of PCR cycles to amplify the amount of converted-viral-RNA that was originally in it so that it can be detected.
The problem with using polymerase chain reaction to test for viruses is two-fold.
- The bits of genetic material whose amount is being amplified ARE NOT viruses. They’re just small segments of the inert genetic material found inside a virus’s shell. Without the shell, they don’t have any ability to infect a cell and reproduce. The PCR test, so to speak, doesn’t detect “live” viruses, at best it only detects their “remains.” And even that depends on assuming that the testing company has accurately sequenced the COVID-19 virus’s genetic code and identified a small segment that’s unique to it and will remain so as the virus mutates.
- But even supposing you’re willing to trust that they’ve really done all that, the detection of viral remains involves massively amplifying the amount in the original sample by running it through successive PCR cycles. And nothing about the PCR test itself will tell you if there was actually any “live” virus in the original sample at all, let alone how much.
As the CDC itself has noted:
[R]ecovered patients can continue to have [the COVID-19 virus’s] RNA detected in their upper respiratory specimens for up to 12 weeks” after the onset of symptoms.
The actual “live” virus, on the other hand, hasn’t been found beyond “3 weeks after symptom onset.”
Moreover, even if you could be sure that you’d found sufficient quantities of viral remains to indicate the presence of the virus itself, determining how much is crucial.
You have all kinds of minute viral traces in your body that never rise to the level of infection. Even if PCR testing could tell you that the remains it amplified indicate the presence of a “live” virus, you’d still need to know the amount or viral load in order to tell if the person the sample came from has enough to be classified as infected.
That’s why Mullis objected to turning the process he created for generating research samples into a test for viruses by famously saying:
Quantitative PCR is an oxymoron.
PCR can’t detect quantity. At best, it can detect the presence of a virus, not the amount. And without knowing the amount, there’s no way to tell if the person being tested is infected.
But even detecting the presence of a “live” virus will depend upon inferring it’s in the sample from the detection of viral remains. And that’s the source of the massive amount of bad PCR diagnoses reported in the New York Times. If you run a sample with minute traces of viral remains through enough cycles, you’ll wind up with enough to be detected.
And it turns out that laboratories have been running the samples their testing through so many cycles that ones without nearly enough viral remains to indicate the presence of a live virus are, nonetheless, being amplified enough to produce a positive test result.
Moreover, the CDC has been telling them to do it…
…The 3rd and final installment is up.
Same Red-time.
Same Red-channel
If you missed Part 1 or need another look, you can find it here…
PART 3
“The urge to save humanity is almost always a false face for the urge to rule it.”
― H.L. Mencken
***
In the previous entry, we learned how a process invented to increase the size of research samples of DNA called polymerase chain reaction is used to test for viruses even though the guy who received a Nobel Prize for inventing it said using it that way doesn’t work.
Kary Mullis’s PCR process takes segments of DNA through a “cycle” that doubles the amount. If you run a single segment of DNA through just 40 cycles, you’ll end up with 1 x 240, which is over a trillion copies. Remember that number, it’s going to be important later.
We also saw that the COVID-19 virus, like any other virus, is just some genetic code surrounded by a shell that acts as a “Trojan horse,” allowing the virus to invade the cells of living organisms. Once inside, the genetic code exits the shell, hijacking the cell’s functions to make it produce more copies of the virus.
The genetic code inside the COVID-19 virus’s shell is RNA. So, since the PCR cycle only works on DNA, before a sample is tested for COVID-19 another process is used to convert the former into the latter. Once that’s done, the sample is run through a number of PCR cycles to amplify the amount of any converted-viral-RNA that was originally in it so there’s enough be detected.
But two factors are responsible for creating the massive unreliability of PCR testing that, as we saw in part 1, the New York Times reported on but downplayed to push for mass testing of a different kind.
- The bits of genetic material whose amount is being amplified ARE NOT viruses. They’re just small segments of inert genetic material found inside a virus’s shell. Without the shell, they don’t have any ability to infect a cell and reproduce. The PCR test doesn’t detect “live” viruses, at best it only detects their “remains.”
- The detection of viral remains involves massively amplifying the amount in the original sample by running it through successive PCR cycles. And nothing about the PCR test itself will tell you if there was actually any “live” virus in the original sample.
The number of PCR cycles it takes to amplify a sample containing viral remains to the point where they can be detected is called its cycle threshold.
And if the New York Times were interested in producing journalism rather than shilling for mandatory testing, they would have focused their whole story on something you have to read three-fourths of the way in to even find out.
The Food and Drug Administration said in an emailed statement that it does not specify the cycle threshold ranges used to determine who is positive, and that “commercial manufacturers and laboratories set their own.”
The Centers for Disease Control and Prevention said it is examining the use of cycle threshold measures “for policy decisions.” The agency said it would need to collaborate with the F.D.A. and with device manufacturers to ensure the measures “can be used properly and with assurance that we know what they mean.”
So the FDA and CDC have spent months hyping a test that involves amplifying tiny samples of viral remains until there’s enough to detect. But, according to the New York Times, there are no rules or even any guidelines for how much amplification the testing companies do.
Even though obviously, the more positive test results they churn out, the more downstream business they’ll get from people who are worried because they had contact with someone that tested positive and the general increased concern over the virus.
And, of course, the Times neglected to mention any of that but, instead, focused on pushing for continuing to mass test for COVID-19 but using a different test.
As we saw in the previous entry, they also failed to mention that, since any test will have a false positive rate, regardless of the one that’s used, mass testing will mean that an alarming number of bogus COVID-19 cases will continue to be reported every single day from now til eternity even after the virus has run its course.
Convenient huh?
What the Times says about the unreliability of PCR testing, however, significantly understates how badly the cycling process is being abused to inflate the number of positive test results.
Their article says that most testing companies run the samples they receive through 40 cycles. As we saw above, that means any genetic material in them is being multiplied over a trillion times. We’re told that a few companies run samples through only 37 cycles, which is still multiplying the amount of converted viral-RNA by a factor of almost 140 billion.
The New York Times goes on to say that the “C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles.” But, this is a deceptive way of stating what the CDC’s data shows that significantly understates how using 40 or even 37 cycles is going to result in massive amounts of positive diagnoses that ought to be negative.
The CDC didn’t just have “extreme difficulty” finding any live virus in samples whose cycle threshold was above 33. They were straight-up unable to find any. Moreover, they frequently detected no live virus even in samples that had lower cycle thresholds.
But the worst is yet to come.
Though the CDC replied to the Times by saying they were “examining the use of cycle threshold measures for policy decisions,” the New York Times either didn’t know or didn’t want you to know that the CDC already has guidelines that recommend … wait for it… 40 amplification cycles. Even though their own researchers were unable to find any live virus in samples with a cycling threshold greater than 33!
That’s right folks. The CDC issued guidelines for COVID-19 testing that their own research showed were bound to mean that a lot of people not infected by the virus would get back test results falsely saying they were.
Moreover, even running samples through the 33 cycles the New York Times mentions as the cutoff point in the CDC’s research appears to be way too much amplification.
One paper the CDC sites reports finding no “live” virus in any samples whose cycle threshold is greater than 24. And, even the CDC found a lot more samples that had no live virus than they did samples that did for cycle thresholds between 24 and 33.
Moreover, a pooled analysis of several different studies by a team of researchers at Oxford also concluded that positive PCR test results from samples with cycle thresholds over 24 shouldn’t be taken to indicate the presence of any actual virus.
The upshot of all of this is that the 40 amplification cycles recommended by the CDC and used in the majority of U.S labs looks like it will generate a lot more bogus positive test results than even the New York Times said.
The Times claimed that around 90% of samples taken from a set of positive tests that used 40 cycles were really negative because, when they were run through only 30 cycles, no viral remains were detected.
But given that 30 cycles also appear to be way too much amplification, it’s likely that a lot more than just 90% were actually bogus. Who knows how few positive diagnoses would have been verified if they’d used the much lower 24 number of amplifying cycles recommended by the Oxford team and above which the other research cited by the CDC found no live virus.
Moreover, though that other research did at least sometimes find actual virus in some samples with cycle thresholds at or below 24, they still frequently found none. Meaning that, so far as the available research goes, positive PCR test results appear to never be very reliable regardless of how few amplification cycles are used.
But it gets even worse. All the studies cited by the CDC were done only on people with symptoms. And it turns out that the number of days after onset seems to have a huge effect on whether positive PCR test results are reliable.
According to that study the CDC cited that found no virus at cycle thresholds above 24, if a sample testing positive is taken more than seven days after the onset of symptoms, the probability that the test is indicating the presence of live virus is… wait for it…. zero.
But even positive test results from samples taken within 7 days of the onset of symptoms don’t turn out to be very reliable. The study only found a 40% or less chance of discovering any live virus in samples testing positive for viral remains that were taken on any of the first seven days after symptom onset except the third and fourth. And the ones taken on the third day only had an 80% chance of containing any virus while the ones taken on the fourth only had a 70% chance.
Even for people with symptoms, the research seems to show that regardless of how few cycles you use the PCR test is going to diagnose a lot of people who aren’t actually infected with the COVID-19 virus as positive.
And, putting samples through 40 cycles as labs are doing on the CDC’s recommendation is likely to yield a whole lot more bogus positive results than the upper bound of 90 percent the Times suggests.
But what’s worse for the regime of mass testing is that none of these studies was done on asymptomatic patients at all. So we have no reason whatsoever to believe that PCR testing is ever reliable for discovering infections in people who don’t show symptoms.
Remember:
- The study which kept track of the amount of time after symptom onset samples were taken found no live virus in samples testing positive taken more than 7 days after symptoms began.
- The CDC didn’t find any virus in most samples that tested positive after being run through more than 24 cycles. The other study found no virus in any samples with a cycle threshold greater than 24. And the Oxford pooled analysis also found that more than 24 amplification cycles is too many.
Given that most labs in the U.S are running samples through 40 amplification cycles and the few that aren’t are amplifying them 37 times, as hard as it is to believe, it’s very possible that, for all intents and purposes, no one in America who tested positive but didn’t have symptoms was really infected.
And even if some were, the percentage who weren’t is likely to be a lot more than the 90% upper bound suggested by the New York Times.
Moreover, given the available research, a positive PCR test isn’t even a reliable indicator of COVID-19 infection even if you do have symptoms. It wouldn’t be at all surprising if most of the people with symptoms who’ve been led to believe they have COVID-19 by a positive PCR test really have something else.
In short, all the available research seems to indicate that positive PCR test results are utterly meaningless.
It turns out that the guy who won a Nobel Prize for inventing the process was right.
And, since PCR tests are the standard diagnostic tool that have been used to detect COVID-19 infection, all the data we’ve been given is worthless too. We don’t have a clue how many people have really been infected with the COVID-19 virus or what it’s fatality rate is.
The numbers the medical bureaucrats in charge have been throwing at us might as well have come from a Ouija board.
But there’s something that’s, in a way, even more scandalous going on here.
The CDC was hyping PCR tests for COVID before any of this research was even done. They were also using the results to compile data about it which was then used to scare the public and justify the never-before-seen widespread adoption of extreme measures to slow down its spread.
Clearly someone needs to investigate why the CDC recommended that COVID testing labs run samples through 40 amplification cycles.
Why PCR testing is even still being used to generate data that keeps the country in a state of panic when it’s clearly worthless is another thing that obviously needs to be looked into seriously.
But a more basic question is why PCR tests were being hyped as “the gold standard” for COVID-19 detection before any testing was done to verify that claim when they don’t even detect the virus.
The American people have been frightened into surrendering their most basic liberties based on a test that both Anthony Fauci and CDC director Robert Redfield had to know there was no reason to think was at all reliable.
And once the research showed that the test is likely falsely diagnosing millions of Americans who don’t have COVID-19 with the virus, they not only did nothing to end its use, they continued scaring us with its results.
We’re talking about perhaps the greatest political scandal in all of history. And it’s about time someone with authority found out what those responsible were trying to accomplish and make sure that, whatever it was, they’re made to pay the steep price justice demands.
Way too much damage was inflicted and way too many lies were told to let this pass.
Finis
…If you missed part 1 or need another look, you can find it here…
Part 2 can be found here.
TOPICS: Health/Medicine; Science; Society
KEYWORDS: covid; covid19; diagnosis; newyorktimes; testing
To: SeekAndFind
what does that do to the positivity rates ?
are we all going to die?
eventually, yes.
2
posted on
09/03/2020 12:33:33 PM PDT
by
teeman8r
To: SeekAndFind
The false positives are being used to drive out healthcare workers. The CDC is unconstitutionally mandating weekly testing of all healthcare workers so that they can fire them. Healthcare companies think this is a reasonable mandate but fail to see the evil plan unfolding. Democrats have been creating temporary agencies to fill in for those healthcare workers that are pushed out.
3
posted on
09/03/2020 12:36:45 PM PDT
by
CodeToad
(Arm Up! They Have!)
To: teeman8r
The link to Part 2 is not working.
4
posted on
09/03/2020 12:44:30 PM PDT
by
dsc
(We are competing against Soros money poured onto a hive mentality.)
To: SeekAndFind
This thing is not even the flu, bro.
2 years ago, flu killed something like 60,000 people. I say COVID-19 has killed fewer than 20,000.
5
posted on
09/03/2020 12:46:42 PM PDT
by
ClearCase_guy
(If White Privilege is real, why did Elizabeth Warren lie about being an Indian?)
To: SeekAndFind
Perhaps the NYT is beginning to see its role in saving New York City from the political tyrants who are desperately trying to destroy it ... as well as anyone who still lives there.
6
posted on
09/03/2020 12:46:55 PM PDT
by
glennaro
(Democrat/Left Party core principle: You can control anyone if you frighten them enough.)
To: SeekAndFind
When we were first hit with the media pandemic, there was a poster on FR who was concerned about this reality with the PCR tests.
Also, remember those fantastic drive through tests in Korea and ???? their fantastic cure rates and other Eastern Asia countries.
Easy to cure if there was no Covid~19.
7
posted on
09/03/2020 1:04:05 PM PDT
by
Grampa Dave
(11/3/2020! VOTE FOR JOBS! NOT RIOTING BLM/ANTIFA/DEM/MOBS! POLICE FOR US! NOT JUST FOR THE ELITE!!!)
To: SeekAndFind
This is how the world ends...not with a whimper or a bang...but with agendas.
To: SeekAndFind
The end result of this will be that fewer people actually had it than reportedly died from it. It’s been more effective than the Russia and Ukraine hoaxes, you have to give them that. It was enough to give a man with dementia a brief lead in some fake polls.
9
posted on
09/03/2020 1:13:40 PM PDT
by
cdcdawg
(Biden has dementia.)
To: SeekAndFind
10
posted on
09/03/2020 1:24:54 PM PDT
by
Magnum44
(My comprehensive terrorism plan: Hunt them down and kill them.)
To: ClearCase_guy
So what killed the other ~170,000 people who are dead unexpectedly? There’s a huge jump in excess deaths this year around the world, but particularly in the US. What’s causing that if it isn’t the global pandemic that’s listed on the death certificates?
11
posted on
09/03/2020 1:48:03 PM PDT
by
2aProtectsTheRest
(The media is banging the fear drum enough. Don't help them do it.)
To: SeekAndFind
Every false positive is a “case”. The number the DeepState touts is “cases”. Not “people with symptoms”. Not “people who need to be treated”. Not “Intensive care traffic”. And certainly not “Deaths”. Use the biggest number to scare the most people. And Karens everywhere are happy to chase us around and nag us about masks.
12
posted on
09/03/2020 2:02:18 PM PDT
by
motor_racer
(Who will bell the cat?)
To: 2aProtectsTheRest
On average, what is the yearly total number of deaths, for *ANY* reason, in the US?
I’m asking because I don’t know. But that seems a logical place to start.
To: AFreeBird
To: AFreeBird

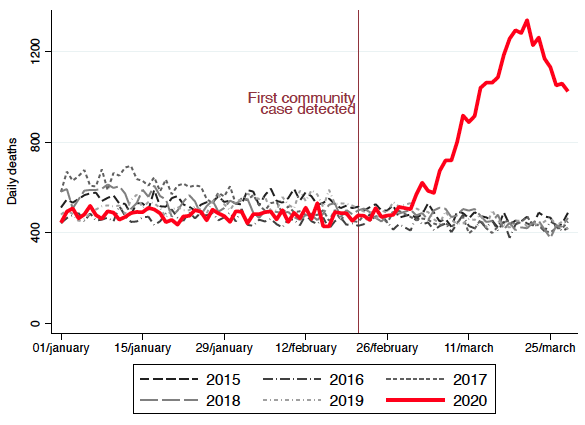
Here's the weekly stats for the entire year leading up 'til now: Excess Deaths. We've been well over the normal expected number of deaths every single week since March. Keep in mind that just over half of all jurisdictions (mostly state and local health departments) report their data to the CDC within 10 days, so much of the data for July is incomplete and will look worse as time goes on and more data arrives.
15
posted on
09/03/2020 2:35:04 PM PDT
by
2aProtectsTheRest
(The media is banging the fear drum enough. Don't help them do it.)
To: SeekAndFind; All
Whoever read this piece, please raise your hand.
Seriously, is there an executive summary that states something like this: “90% of reported cases is total BS.”
16
posted on
09/03/2020 3:02:51 PM PDT
by
Cobra64
(Common sense isnÂ’t common anymore.)
To: SeekAndFind
17
posted on
09/03/2020 3:56:17 PM PDT
by
faucetman
(Just the facts, ma'am, Just the facts)
To: AFreeBird
To: Cobra64
I read it. I know the science behind this test. This type of test is not new. It’s based on PCR, invented by Kary Mullis. The fact that Kary Mullis didn’t think this application could work doesn’t mean much; the technology has advanced quite a bit since 1983.
The short version is the test detects the viral genome. Obviously it’s highly unlikely you’d have this viral genome unless you were exposed. But how infected are you? How much live virus do you have? That’s what these studies are revealing - there may be a small window with which to use the test to detect “a hot one”. That seems to be a cycle threshold of <24. The fact that the CDC says to do 40 cycles does not mean they are advocating a high false positive rate. The test needs to be run that long to ensure the controls (the samples that are supposed to be negative) do not amplify and look positive at all. That’s not a conspiracy - that’s ensuring assay validity.
The clincher is “are you detecting SARS-CoV-19 or something that looks like it?” There is more than one design to fish out the virus, and the designs the CDC made initially were bad. Right now I don’t know if labs are required to use the (fixed) CDC-chosen designs, or can develop their own. Having a test available so quickly means less time to check that it’s truly specific. There’s more than one test in the world, some may be better than others. Testing asymptomatic people does not help answer that question.
The science is fine, the test is real, it can be a good tool. I do think it’s ok to question whether the tool is being used appropriately. If there is truly no treatment then I’m not sure why you’d test. If there’s no treatment AND no illness (symptoms) then that does seem like a waste of time.
I could be wrong.
To: ClearCase_guy
The flu never kills that many a year. For around 30 years the stat have conflated pneumonia and all colds are lumped together. I’ve seen convincing estimates that put the real numbers of flu alone without underlying comorbidities at under a 1000 a year. Sounds crazy to the average person given the polluted well of information out there.
20
posted on
09/03/2020 6:18:15 PM PDT
by
Sheapdog
(Chew the meat, spit out the bones - FUBO - Come and get me)
Disclaimer:
Opinions posted on Free Republic are those of the individual
posters and do not necessarily represent the opinion of Free Republic or its
management. All materials posted herein are protected by copyright law and the
exemption for fair use of copyrighted works.
FreeRepublic.com is powered by software copyright 2000-2008 John Robinson