Posted on 05/10/2026 6:35:18 AM PDT by MtnClimber
Medicaid is the joint federal/state program that provides free medical care to the poor and near-poor in the U.S. Who could be against that?
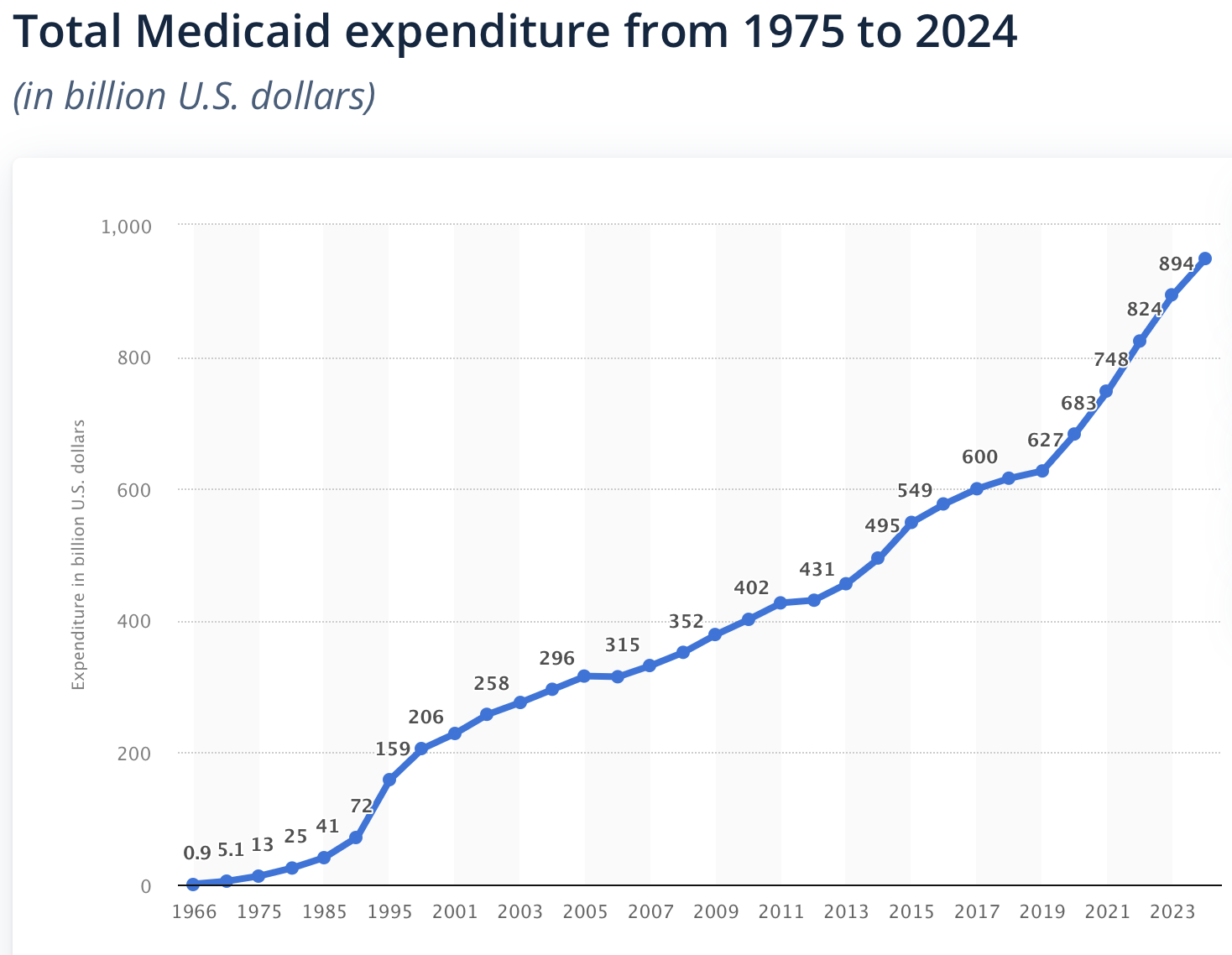
A website called Statista collects data on various subjects of interest and presents them in useful charts. One subject is the total federal plus state spending on the Medicaid program by year since inception of the program back in the 1960s through the latest year of 2024. Here is that chart:
Looking at the chart, a few things leap out. One is rapid and unbroken growth year after year from the beginning up to the most recent year. Another is two particularly rapid periods of growth, first in the 1990s (Bill Clinton was President), and then again in the most recent period of 2020-2024. That last five-year period began in the last year of Trump’s first term (the pandemic year), but then continued throughout the four years of the Biden term. Between the end of 2019 through 2024 the program grew from $627 billion to $949 billion. That’s more than a 50% increase in 5 years, and more than an 8% compound annual rate of growth. The word “unsustainable” doesn’t begin to describe it.
When you think of medical care for the poor, you likely have a mental picture of what all this money is paying for. Probably, your mental picture involves hospitals, doctors, nurses, injuries, diseases, treatments and pharmaceuticals. But how much of the Medicaid spending — and particularly of the recent explosion in Medicaid spending — falls in those categories?
We are recently learning that much or even most of the recent cost explosion falls into other categories that have come under the Medicaid spending umbrella by reason of various “waivers,” and that do not involve hospitals or doctors or medical professionals or medical treatments. Major examples include: in-home assistance, often provided by family members, for things like cooking and housekeeping; transportation to medical appointments; palliative end-of-life care, again often provided in the home (sometimes called “hospice”); autism counseling; and more.
Any of these services could well be legitimate in many cases. But as people have started to look at and publicize exploding expenditures in these categories over the past several years, we learn of one situation after another where the spending appears to exceed anything that could possibly be legitimate. And almost all of the provision of these services is supposedly taking place in homes or other personal spaces where it is difficult to impossible to check if the service is actually being provided.
For today I’ll provide just a few examples recently in the news.
In about 2023 initial news reports indicated that somehow there were some 1800 hospices operating in the Los Angeles area, constituting approximately 6 times the per capita level of such businesses elsewhere in the country. In March, CBS News investigated what they called “ground zero for hospice fraud” in Los Angeles. Excerpt:
Three years ago, California’s state auditor sounded the alarm that Los Angeles County had seen a 1,500% increase in hospice companies since 2010 – more than six times the national average relative to its elderly population. . . . The state says it proceeded to investigate and revoke the licenses of 280 hospices. But since then, the problem has continued to fester. CBS News examined the business and financial records of every hospice currently operating in LA County, applying the same indicators identified by the state. Indications of fraud have not stopped. In fact, they’ve grown.
(Note that the hospice fraud issue involves the Medicare program, as well as Medicaid.)
In the area of in-home personal services, a reporter named Luke Rosiak at the Daily Wire is just out with a three-part series involving what appears to be widespread fraud in the Columbus, Ohio area. Here are links to Part 1 (May 4), Part 2 (May 5), and Part 3 (May 7). This alleged fraud, like the Minnesota free-meals scandal, involves a large community of almost entirely Somali-Americans. The entire series is well worth your attention. Besides revealing specific instances of fraud, the series goes into how the level of spending is completely implausible given the population to be served. Here is an indicative excerpt from Part 2:
The seven buildings along East Dublin Granville Road in Columbus, Ohio, are filled with hundreds of office suites, all owned by a company named Cordoba Real Estate. A large majority of the tenants in the buildings bill Medicaid, the taxpayer-funded medical program for the impoverished, as a “home health care” business that provides low-skilled, usually non-medical care to elderly or disabled people. The Daily Wire has spent weeks analyzing Medicaid data released by the Trump administration’s Department of Government Efficiency in an effort to weed out wasteful government spending. The buildings owned by Cordoba stuck out, each housing dozens of businesses that bill Medicaid. In all, the Cordoba-owned buildings in Columbus housed 288 businesses registered with Medicaid, The Daily Wire investigation found. Together, they charged taxpayers more than a quarter of a billion dollars between 2018 and 2024. That’s in a city where only 6,273 people 75 or older are on Medicaid.
And don’t get the idea that explosive growth of Medicaid spending on home health aides is confined to a few Somali communities in the Midwest. New York State has one of the most out-of-control Medicaid-funded home health aide programs. Here is an April 2025 report on the issue from the Empire Center. Excerpt:
New York’s home health employment is continuing to soar, growing by 57,000 jobs or 10 percent from 2023 to 2024, according to newly released data from the U.S. Bureau of Labor Statistics. The state’s workforce of home health and personal care aides grew to an estimated 623,000 as of May 2024, according to BLS’s Occupational and Occupational Employment and Wage Statistics, an annual survey posted Tuesday. That equated to 171 aides per 1,000 residents aged 65 or older, which was the highest rate in the U.S. – 153 percent higher than the national average and 24 percent ahead of the No. 2 state, California.
New York State has only about 10 million jobs total, so 623,000 of these home health aide jobs is more than 6% of all jobs in the state. Are all these people doing legitimate work, or are they just taking advantage of the taxpayers to get paid for hanging out at home with mom? How could you tell?
Autism counseling is another big area. Autism is something without any clear definition, or any good metric for determining if counseling does any good. As one example among many, here is a January 2026 report from the HHS Inspector General about improper payments in the small state of Maine. Excerpt:
The U.S. Department of Health and Human Services Office of Inspector General (HHS-OIG) has released an audit report revealing that Maine made at least $45.6 million in improper fee-for-service Medicaid payments for rehabilitative and community support (RCS) services provided to children diagnosed with autism. . . . In the span of five years, Medicaid payments for RCS services in Maine grew significantly, from $52.2 million in 2019 to $80.6 million in 2023.
While we have barely been looking, the Medicaid program has morphed from medical care to widespread payments for aides and personal services provided by non-professionals. Cooking? Housecleaning? No problem, the taxpayers will pick that up.
|
Click here: to donate by Credit Card Or here: to donate by PayPal Or by mail to: Free Republic, LLC - PO Box 9771 - Fresno, CA 93794 Thank you very much and God bless you. |
Points to be addressed, expanded:
“recent cost explosion in other categories under the Medicaid umbrella”
“Keeping track of it could be a Real job for AI”
“they enrolled unsuspecting, healthy people”
“rely on the physician’s honesty”
“Medicare/Medicaid dual eligibles are a large percentage”
“fraud contributes to the problem, but not the primary cause”
“big bucks in NICU and end of life care”
“90% of it goes to fund the government infrastructure”
“Hospital costs can be reduced by splitting most hospitals”
“primary cost: pharma, hospitals, doctors, medical devices, insurance not addressed.”
“hospices are required by federal law to have a physical office.”
They’re popping out babies left and right, have older generations here now, and are IIRC required by federal law to get emergency care gratis.
Send them home!
You have monopolies especially in pharma, very tight restrictions crossing national borders for anything, caps on how many doctors get licensed (did you even know they do this?), alternatives are choked out (example midwives), insurances get semi-monopolies because there are rules in place on who can do business in what state (literally government limiting the competition for them)...
Just one example to prove my point: https://www.openhealthpolicy.com/p/medical-residency-slots-congress
Instead on focusing on supply (Reagan's approach macro economically to fire up the economy was supply oriented, and it worked!!!), they focused almost entirely on demand, like government bureaucracies tends to do, like socialists (the political left) tend to do.
Guess who created this system? Government bureaucracy and a bunch of more left leaning politicians who pandered to the insurance companies, doctors, hospitals and pharma so they don't face resistance.
Instead of leaning on pharma, insurance, doctors and hospitals, they basically just restricted the care “you” the consumer gets. Of course that is NOT going to fix the problem with rising costs, and that too was predictable even as the MSM cheered on Obama care (anything Obama did was awesome according to the US MSM. He could have farted, and the MSM would have reported about the sweet summer smell of flowers).
The solution is not to lean on the cost drivers by imposing cost caps/mandates (more communist thinking). The solution is to create a truly competitive market.
“They’re popping out babies left and right”
Invader Jr. will get a K-12 education at a cost of $200,000 to $550,000, far more than his Medicaid & EMTALA cost.
For health care, bring on market force:
1. Break most hospitals into two highly competitive entities.
2. Convert other hospitals into real estate leasing entities with competing surgical suites and nursing wings.
3. Separate out drug coverage so hospital systems can run care coverage systems and cut out insurance company overhead and meddlers.
4. Create interstate drug plans that don’t have to pay what the drugmaker wants for every drug. To qualify for exchange listing and federal subsidies, they would have to most (~80% or more) in all important types (large volume recombinant, small volume recombinant, breakthroughs under patent, etc.). Group and exchange plans to offer time-limited vouchers at plan set amounts for out-of-formulary drugs. Voucher plans would have variable premiums. Plans without minimums (or vouchers) could be vended directly to individuals and families.
5. These plans would be all the doctors (and AI) prescribe for formulary drugs with co-pays equal to manufacturing cost
6. Have drug patents limited by government sourced product revenue and overall domestic government health care spending and not by time [so drug companies have an incentive to minimize government health care funding].
7. Require Kirchoff patent collapse to a single entity upon FDA marketing approval of a covered entity.
8. Reform medical education, breaking down medicine and dentistry into simpler chunks and start it in the first year of college
9. Replace most primary care doctoring with AI.
(Insurers would pay human doctors to confirm AI diagnosis, orders for expensive tests[MRI, genetic], prescribe radiation imaging[CT, PET, X-ray]/treatment, and voucher/government co-pay drugs. Other human doctor care would be private pay.)
10. Radioisotope-related care would be at international airport centers
Here’s the advantage for why mandates and cost caps win over true long term structural reforms.
The mandate is simple to understand, easy to implement, and it’s effect immediate.
For a politician, you can show results from one year to the next. Heck, from one month to the next.
True structural changes will take time, years. But those changes are real, not just some temporary populist Mamdani style move which long term digs us into an even deeper hole which his rent control measures will surely cause. Mamdani in NYC is the perfect example of why mandates and idiotic cost controls win out over true structural changes that improve things long term.
“recent cost explosion in other categories under the Medicaid umbrella”
Other categories? IT company swamp now paid to avoid pinning the blame on them and pinning it on somebody else.
“Keeping track of it could be a Real job for AI”
AI is only as good as the data it is fed; not unique to AI. The Deloitte eligibility problem is the quality of the data.
“they enrolled unsuspecting, healthy people”
Deloitte does the enrolling/eligibility in most states, in all the big states.
“rely on the physician’s honesty”
And can we rely on the honesty of Deloitte?
“Medicare/Medicaid dual eligibles are a large percentage”
“big bucks in NICU and end of life care”
Medicaid is barbells, heavy in elderly, in women of pregnancy age, in NICU newborns, in those with bad lifestyle choices.
It is expensive to keep the elderly alive ... one more month. Most newborn expense is due to the bad lifestyle of parents. If excess sugar is added to the lifestyle choices then lifestyle is the overwhelming cost of Medicaid.
Bad lifestyle choices of tobacco, alcohol, drugs, STDs are the biggest preventable big expense. Set a policy: No person age 18 with bad lifestyle choice can apply for Medicaid. Increment it each year to 1 year older in age.. 19, then 20, etc. If a person wants to make bad lifestyle choices, he is free to do so. But don’t expect the taxpayer to pay for those bad lifestyle choices.
“fraud contributes to the problem, but not the primary cause”
“90% of it goes to fund the government infrastructure”
Employee bureaucrats are obvious. Not so obvious is the swamp of IT and consulting companies that devise ways to spend more money. Accenture taught me: If centralized, de-centralize. If de-centralized, centralize. Whatever the current way is, recommend and do the opposite. That will generate the most money for consultants. This pre-Trump policy continues under Trump/RFK/OZ.
“Hospital costs can be reduced by splitting most hospitals”
Metro Hospitals are paid a higher rate than Rural hospitals for the same procedure. To pay for big new metro Medicaid Centers patients must be brought in from the rural areas to fill the beds and keep the staff busy. The Metro Hospitals buy up the rural hospitals and use them to feed rural patients to the big Metro Hospital where Medicaid will pay more per patient. As number of patients in rural hospitals declines, the rural hospital loses its specialty departments, which further speeds the transit of patients to the big Metro hospital.
“primary cost: pharma, hospitals, doctors, medical devices, insurance not addressed.” Don’t forget government as a primary cost. It is state & federal regulation of doctors, hospitals, everything medical that raises the cost. And don’t forget the IT and other consulting companies in the swamp: Deloitte, Gainwell, Acentra, Optum, Accenture, GDIT, etal. Deloitte is outright FRAUD. The WASTE FRAUD ABUSE at Gainwell is mostly in processing the dirty data it receives from Deloitte.
“hospices are required by federal law to have a physical office.”
Medicaid & most states require ALL medical providers to have a Physical location where services are delivered. Most states require this be a licensed location that is physically inspected for cleanliness, etc. In GA and other states, Medicaid now bypasses that and pays for instate providers not in that licensed location, contrary to state law. Government bureaucrats are slow to come up with modern systems to handle this.
Add to your list:
MANY prescription drugs are only prescription so pharma and doctors can make money. There is NO RATIONAL MEDICAL REASON for this.
Yes, AI could do a quick screening (make sure there are no issues), informational session (how to use, manage expectations), and record keeping.
Insulin (someone that has been shooting insulin for 20 years knows what to do), Antibiotics, proton pump inhibitors, GLP-1... all this stuff should be as simple as scanning your ID (over 18) and chatting with an AI assistant for 5 minutes.
Think about this irony. Big pharma get many of their precursors chemicals and biological substances from China. Much of our medication is made with things that come from China, the ingredients so to speak. But firms in China, Brazil, Mexico, Turkey can’t sell the pharma in the US directly.
Example: https://www.renalandurologynews.com/news/u-s-drug-supply-deeply-dependent-on-chinese-ingredients/
Could you imagine what sort of pressure that would be on costs if you had international movement of medication no differently than a T-shit or swimming trunks sold on Amazon? https://worldpopulationreview.com/country-rankings/cost-of-insulin-by-country
The costs of medication would plummet!
—
The reason why we have never seen TRUE solutions to rising health care costs is because DC is controlled by money / special interests.
I have been practicing since 1974, and I have absolutely no idea what will follow the collapse of what exists now.
I admit to not reading the article. Does it mention how much actually goes to medical care for the most vulnerable?
No. If the monitoring cannot determine fraud then how can it determine proper expenses?
I just hope I don’t go to the doctor for stitches and get a prescription for MAID.
I think widespread MAID is a lot less likely than no doctor to go to.
kwtx.com
By Laura Geller, Adam Yamaguchi,
Rachel Gold, Graham Kates
Mar. 23, 2026
Official State records show 89 hospice companies
at Los Angeles’ Merabi Professional Medical Plaza
(CBS News) - The Merabi Professional Medical Plaza, a small three-story,
32,000 square foot stucco and glass office building in LA, rents space to
<><>a hair salon, a law office,
<><>a modeling agency, a realty corporation
<><>and 89 licensed hospice companies.
<><>this adds up to more rental space than actually exists
The Merabi building is among the most extreme cases of “clustering” —
a grouping of large numbers of hospices considered a major red flag for potential fraud.
<><>The Van Nuys address, “Merabi Plaza”
<><>appears dozens of times in official state records for “licensed hospice companies.”
<><>Merabi’s building directory lining hallways lists numerous hospice agencies.
<><>landlord Merabi says he himself lists only 12 hospice agency rentals.
Taxpayers would be interested to know how Merabi handled the discrepancy on his tax return,
Auditors said the Merabi building clustering of so many firms raised concerns because it suggests that “the number of agencies in these areas likely exceeds the number of patients who need services.”
Concerns about clustering appear in a 2022 California State Auditor’s report, which found that Los Angeles County had experienced a 1,500% increase in hospice companies countywide since 2010. That’s six times more hospice providers than the national average, relative to the county’s elderly population.
Auditors said other warning signs for potential fraud include
<><>multiple hospices in one building,
<><>geographic clustering,
<><>low patient counts,
<><>high rates of terminally ill patients later discharged alive,
<><>excessive billing
<><>and staff shared across multiple companies.
CBS News found that 72 of the 89 registered hospices in Merabi Plaza have at least three of the six potential warning signs.
Many of the hospice companies in Marabi Plaza have been billing Medicare for years and collecting reimbursements that come from federal tax dollars. On a recent visit, CBS News encountered the landlord, Kambiz Merabi. He said officials from Medicare came there two years ago specifically looking for hospice agencies. Merabi said the businesses appear to be legitimate – noting that his rental tenants are required to provide standard documentation that shows they are valid.
“I’m not a police or keeper of what they do, how they do business,” Merabi glibly said. Merabi was not forthcoming about how he handled the discrepancy on his tax returns.
Merabi said the numbers that appear in government records differ from those on his tenant list. He shows only 12 hospice companies operating in his building. Merabi explained that a number of the agencies had recently “moved.” Public records don’t yet reflect that, and hospices are required to notify authorities if they move.
Advocates say the discrepancy raises questions about what they call “ghost hospices.” Those are paper companies that bill the taxpayers for patients, and pocket massive amounts of tax dollars even if they don’t actually provide any real care.
Copyright 2026 CBS. All rights reserved.
Do you think the politicians will have no doctor to go to?
The Merabi Organization Group, LLC (MOG) is not a publicly held company; it is a privately owned family real estate entity.
MOG is a family-owned entity, specializing in the ownership and operation of luxury residential, office, retail, and hospitality properties, primarily in New York City and Los Angeles. The company is led by older brother, Chairman Nasser J. Merabi and operated by a team including younger brother Kambiz Merabi.
It should not be confused with [sister Nadine Merabi Limited], a separate private limited Merabi company in the fashion industry.
The Merabi Organization Group focuses on purchasing and transforming mixed-use buildings into Class A luxury spaces, operating as a “private investment company.”
Merabi Organization Group
https://merabi.org
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.