Covid19Crusher
@Covid19Crusher
The clinical trial data below strongly supports the assertion that a very efficacious treatment of Covid-19 has now been found, for all stages of the disease: ivermectin.
https://ivmmeta.com

Posted on 12/24/2020 7:38:19 PM PST by SeekAndFind
The anti-parasite drug ivermectin has recently garnered attention as a drug that could prevent the transmission of COVID-19 and perhaps even treat the symptoms.
The "data show that ivermectin is effectively a 'miracle drug' against COVID-19," Dr. Pierre Kory said in testimony last week in front of the Senate Committee on Homeland Security and Governmental Affairs.
Kory, a pulmonary and critical care specialist at Aurora St. Luke’s Medical Center in Milwaukee, is a member of a group of doctors calling themselves the Front Line Covid-19 Critical Care Alliance. The FLCCC Alliance has published a review of the research that it claims shows that not only can ivermectin prevent COVID-19, it can also improve outcomes for COVID-19 patients.
Yet critics are highly skeptical. Georgi Momekov, a faculty member in the Department of Pharmacology at the University of Sofia in Bulgaria, said the review contains "several flaws [that] significantly limit the possibility to use it as a guide for evidence-based conclusions and practice recommendations."
Indeed, the evolution of perceptions of ivermectin as a COVID-19 remedy has in some ways copied that of hydroxychloroquine. That drug was highly touted as a possible treatment for COVID-19 after President Trump said in March he was taking it. The Food and Drug Administration even gave hydroxychloroquine a compassionate use authorization as a treatment for COVID-19. It later rescinded it after more research showed the drug was not effective at treating the virus.
But Kory claims that the case of ivermectin is different.
"That is a conclusion based on interpretation of a number of trials," Kory told the Washington Examiner. "And the magnitude of the difference between the controls and the intervention with ivermectin is dramatic and large."
(Excerpt) Read more at washingtonexaminer.com ...
Ping for your interest
But research in the laboratory conducted on cell cultures is quite different than actually testing it on human beings. In a journal article reviewing the laboratory research, Momekov concluded that the doses of ivermectin used in the laboratories were too large to be used safely in humans.
"That was a theory that has been completely disproven because every clinical trial shows dramatic effects at standard dosing, the doses that you use for parasites," said Kory.
"The expectations that at the usual doses of ivermectin will behave like an antiviral [in humans] is a theory that is still to be validated in the clinic," replied Momekov.
There have been 11 randomized controlled trials, often considered the gold standard for medical research, of ivermectin’s effect on COVID-19, although only two have been peer reviewed. Some of them seem to have produced impressive results.
One randomized controlled trial in Egypt examined family members of patients who had tested positive for COVID-19. A dose of ivermectin was given to family members twice, on the day of the positive test and one week later. After a two-week follow-up, just over 7% of family members given ivermectin had COVID-19 symptoms versus 58% of those not given the drug.
Other trials have shown that ivermectin works to reduce symptoms in people who have been infected with COVID-19. A study in Iraq, for example, found that among both inpatients and outpatients, those who took ivermectin had their recovery time cut by an average of seven days.
Yet Momekov says that much of this research has serious flaws.
"Most of the randomized controlled trials analyzed by Dr. Kory and colleagues are of small sample sizes," Momekov said. "Trials with small sizes … do not compensate for the need of adequate, robust, randomized controlled trials."
Small sample sizes can lead to biased outcomes, and none of the randomized controlled trials referenced by the FLCCC Alliance have a sample size of more than 400. One has only 62.
Momekov also criticized the FLCCC Alliance for citing "observational" studies, ones that are not randomized controlled trials, to make its case.
Some of those studies have some serious methodological problems. For example, one study in Bangladesh had no control group. Another study in Iraq included 87 patients, only 16 of whom received ivermectin.
Kory, though, is unmoved.
"That’s a very common criticism that I see as physicians assess evidence," said Kory. "Modern physicians are taught to be very, very skeptical — and I’m not saying that is wrong … But there is so much skepticism around claims about new drugs that when you present really compelling data, the first response I see is that 'it’s uncontrolled, not large enough, study design is inadequate.'"
In response to Kory’s testimony, Republican Sens. Ron Johnson of Wisconsin, chairman of the Senate Homeland Security and Governmental Affairs Committee, and Rand Paul of Kentucky sent a letter last Thursday to the National Institutes of Health "to request that federal government expedite its review of early COVID-19 treatment options. Current NIH guidelines do not recommend treatment until patients are sick enough to require hospitalization — at which point, treatment is often too late." One of the treatment options mentioned was ivermectin.
But Momekov thinks expediting ivermectin is a mistake.
“At present, ivermectin should not be used as [a] COVID-19 treatment except in clinical trials, approved by an ethical commission, and with informed consent of the patient,” he said.
There are MDs here that believe in it and others that don’t believe in it.
Until there is a consensus on something that truly works that is readily available at first signs of COVID..... I am on the list of willing to try it.
Even bought my idiotic horse paste in case I can’t get a script.
The problem with this disease is that you have no idea in the beginning if you will be one that has no problem or one that hits the skids at day 5-7. By the time you hit the skids the medicine you should have taken Day 1 may not be as effective.
RE: There are MDs here that believe in it and others that don’t believe in it.
If it were up to me to make the policy decision for the country, I would say — LET PHYCISIANS WHO BELIEVE IN IT BE FREE TO PRESCRIBE THE DRUG AS THEY SEE FIT.
For those who don’t believe in it, nobody is forcing you to use it. Feel free to prescribe what you want.
Yeah just like HCQ. No surprise here. No the proof is in for HCQ and it shows it works great and that many people died needlessly.
I order it from Australia, Nuheart, even with required air freight it way less that I pay here...no prescription necessary.
It’s used for worming horses. I have three hay burners we wormed. The ivermectin for my wife and I is on my desk by my Mac. Right now it’s quercetin, zinc and vitamin D. My body, my choice. IMHO.
If it is truly effective and cheap it will be banned, at least in California and the other Democrat states. Democrats do NOT want the Chinese Flu to go away. It is ushering in their total rule.
not recent, i first heard about this in april or may. Cheap, already labeled for human use....
I bought some at the feed store to have on hand if need be. Is there some protocol to follow with the horse paste?
Agree with you. My body, my choice.
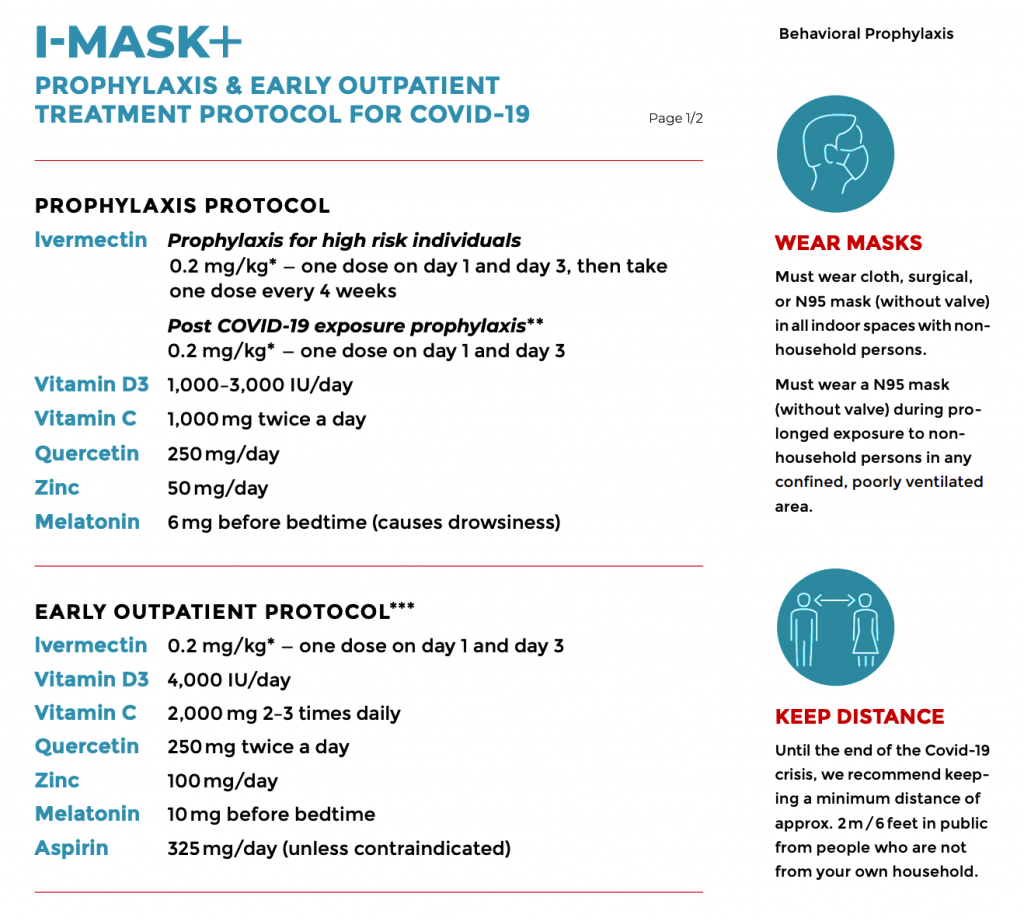
This website actually explains the dosage and the protocol to be used for Ivermectin in conjunction with other vitamins and minerals:
https://covexit.com/a-protocol-for-the-prevention-and-early-treatment-of-covid-19-in-nursing-homes/
my Farm Store had it under lock and key with at least two notices on the glass that it was not for human consumption. The vaccine refrigerator case right beside it with expensive vaccines had no lock and key.
Covid has the same symptoms as the flu so, any reason why these therapies can’t be used for both.
Oh, and I loved the PSA today “A high fever is the first sign of Covid...”
What horrible horrible horrible massaging (I wrote it)
There are a whole host of things that can cause a high fever such as the flu or dengue fever...
I had covid back in March. Used off the shelf ivermectin from TSC. I weigh 260lbs, and I used a half dime sized amount. Symptoms were severe, but cleared up in about 4hrs of treatment. Only side effect was a temporary partial loss of vision in my right eye as a worm that I didn’t even know I had, died and floated to the surface.
So Georgi Momekov, a faculty member in the Department of Pharmacology at the University of Sofia in Bulgaria, doesn’t like Ivermectin for a host of reasons.
Where and how did they find this objector? He’s a “faculty member” — it doesn’t say “professor.” He’s in the Department of Pharmacology, apparently not a researcher in virology. Is his university a major medical research establishment? He is making all the same Fauci /NIH / CDC arguments that the studies are too small or weren’t conducted properly.
Who is this guy and why is he really rejecting Ivermectin?
This strikes me as really peculiar.
Australia has a Covid death rate of only 35 per million but they are one of the most locked down countries too.
.
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.