Skip to comments.
AIDS Infection Rate in U.S. Higher Than Previously Estimated
Washington Post ^
| August 2, 2008
| David Brown
Posted on 08/02/2008 12:22:48 PM PDT by neverdem
Updated federal estimates of the annual number of new HIV infections in the United States, released today, reveal that while the AIDS epidemic here is worse than previously thought, prevention efforts appear to be having some effect.
Even though the number of Americans living with HIV has risen by more than a quarter million people since 1998 -- largely the result of life-extending antiretroviral drugs -- the number of new cases each year has declined slightly over that period. That suggests that a person's likelihood of transmitting the virus to someone else is substantially lower now than it was a decade ago.
The new, if indirect, evidence that prevention programs are paying off was one of the few encouraging findings in an update on the American AIDS epidemic released today by the Centers for Disease Control and Prevention on the eve of the 17th International AIDS Conference, in Mexico City.
"Over 95 percent of people living with HIV are not transmitting to someone else in a given year," said David R. Holtgrave, an expert on AIDS prevention at the Bloomberg School of Public Health at Johns Hopkins University. "What that says is the transmission rate has been kept very low by prevention efforts."
Those include targeting public health messages to high-risk groups, promoting widespread AIDS testing, and getting quick medical care for newly diagnosed cases, which in most cases lowers the person's infectiousness.
The CDC spends about...
--snip--
The epidemic in the black community is distinctly different from the national epidemic.
From 2001 to 2005, 38 percent of the new diagnoses in African Americans were in women, and 46 percent of new infections overall were from heterosexual contact. Among whites during the same period, 16 percent of new infections were in women, and 16 percent were from heterosexual transmission...
(Excerpt) Read more at washingtonpost.com ...
TOPICS: Culture/Society; Government; News/Current Events
KEYWORDS: aids; cdc; health; hiv; hivaids; homosexualagenda; obama; obamatruthfile; prolife; publichealth; riskybehavior
Navigation: use the links below to view more comments.
first previous 1-20 ... 41-60, 61-80, 81-100 ... 121-133 next last
To: xDGx
Nice try.
Roberto Giraldo, MD
(University of Antioquia, Colombia, specialty internal medicine) ; Master of Science in infectious and tropical diseases (U. of London, The London School of Hygiene and Tropical Medicine). Member of South Africa’s Presidential AIDS Advisory Panel.
http://www.rethinkingaids.com/Content/TheBoard/tabid/60/Default.aspx
To: GodGunsGuts; count-your-change; Rudder; TASMANIANRED; xDGx
62
posted on
08/02/2008 4:09:45 PM PDT
by
neverdem
(I'm praying for a Divine Intervention.)
To: GodGunsGuts
Nice try. Roberto Giraldo, MD (University of Antioquia, Colombia, specialty internal medicine) ; Master of Science in infectious and tropical diseases (U. of London, The London School of Hygiene and Tropical Medicine). Member of South Africa’s Presidential AIDS Advisory Panel. http://www.rethinkingaids.com/Content/TheBoard/tabid/60/Default.aspx Don't give me that "nice try" stuff. If you READ what I had posted, the guy is not licensed in the US and works as a tech at the hospital.
http://www.robertogiraldo.com/eng/ResumeShort.html
I don't know of any qualified MD's working as lab techs. YMMV
No Doc Giraldo's at Presby: http://www.nyp.org/
No Doc Giraldo's at Cornell: http://www.med.cornell.edu/cgi-bin/phf
Not really surprised though, considering the quality of his writing.
63
posted on
08/02/2008 4:27:14 PM PDT
by
xDGx
To: neverdem
Why are you bothering me with stuff that ASSUMES that HIV causes AIDS? Save that for the true believers.
To: xDGx
To be honest, the more I dig into Dr. Giraldo background, the more convinced I am that his credentials are solid. I don’t think you can blame him for not being able to practice medicine in the US as he didn’t come over here until close to retirement age, and the “United States requires graduates of foreign programs to study in the U.S. before they can become a doctor in this country.” Having said that, I think his experience uniquely qualifies him to weigh-in on the AIDS debate:
Roberto A. Giraldo
Medical Doctor, Specialist in Internal Medicine with a Major in Infectious Diseases from University of Antioquia, Colombia. Graduated with distinction from the London School of Hygiene and Tropical Medicine, University of London, after obtaining a Master of Science in Clinical Tropical Medicine.
For four decades dedicated to clinical, academic, and research activities regarding different aspects of infectious, tropical, and immunological diseases, in various regions of Colombia, the United States, Europe, and Africa.
Much of his research has been in the field of secondary or acquired immune deficiencies, especially those occurring in developing countries. In 1967 studied, with Professor Jacob Frenckel at the Kansas University Medical Center, Toxoplasma gondii and Pneumocystis carinii infections, as surrogate clinical markers for human immunodeficiency. Also in 1967 studied opportunistic fungal infections with professor Donald Greer at the Centers for Disease Control (CDC) in Kansas City, Kansas. During 1974 and 1975, at the London School of Hygiene and Tropical Medicine, studied the main risk factors for endemic Kaposi’s sarcoma, as a surrogate clinical marker for immune deficiency in African countries.
From 1979 until 1987 worked as a clinician at a remote, rainforest region of Colombia. Here had the opportunity to work shoulder to shoulder with indigenous traditional healers, exploring ways to address a great variety of medical issues related to poverty, malnutrition, immune deficiencies, parasites, and infections.
Independent researcher of AIDS since 1981. Have several publications on AIDS and related conditions. In 1997 published a book— “AIDS and Stressors: AIDS is neither an infectious disease nor is sexually transmitted. It is a toxic-nutritional syndrome caused by the alarming worldwide increment of immunological stressor agents.” The book was published in Spanish in 2002: “SIDA y agentes estresantes: el SIDA no es infeccioso ni se transmite sexualmente. Este es un sindrome toxico-nutricional causado por el alarmante incremento mundial de agentes estresantes para el sistema inmunologico.”
1993 to present work as a technologist in the Laboratories of Clinical Immunology and Molecular diagnosis at the New York Presbyterian Hospital, Weill Cornell Medical Center, in New York City. Here had the opportunity to run and know in detail the Elisa, Western blot and PCR (viral load) tests for HIV.
Since 2000 member of the South African Presidential AIDS Advisory Panel. Advisor of several African countries concerning nutrition and diseases related to poverty. In 2003 presented to 14 Ministers of Health of the Southern African Development Community (SADC) the scientific bases for this proposal: “Nutritional therapy for the treatment and prevention of AIDS.”
Former president of Rethinking AIDS: The International Group for the Scientific Reappraisal of AIDS. Member of the Board of Directors of Health Education AIDS Liaison, HEAL-New York and of the Art and Science Foundation of Medellin, Colombia. Panelist at the South African Presidential AIDS Advisory Panel. Scientific advisor of several non-government organizations in Mexico, Nicaragua, Colombia, Peru, Brazil, Argentina, Chile, Bolivia and Spain.
New York City, 2005
To: GodGunsGuts
66
posted on
08/02/2008 5:03:18 PM PDT
by
xDGx
To: xDGx
==People die because clowns like this claim that HIV is harmless.
Actually, many AIDS victims in Africa die because clowns in the AIDS establishment cling to the fraud that HIV causes AIDS. Read the following. Who knows, you might actually learn something:
http://www.duesberg.com/subject/africa2.html
To: xDGx
*** HIV is highly likely to have been a derivative of SIV. Zoonosis is not uncommon when you have a bunch of people hunting and eating monkeys.***8
Since AIDS is a sexually transmitted disease I figure they were doing something else with the monkeys. ;-D
To: GodGunsGuts
Where is the study and what am I supposed to conclude from this statement from Duesberg’s site? How do you know that the V.A. study “followed scientific protocols” (if you know what those are)? If the CDC is not to be trusted why would I trust the V.A.?
And yes I do say it is a matter (not simple) of pro and con since studies will continue and results and interpretations will differ. For that reason dueling studies is a pointless exercise. I presented a study arguing one way and I'm not sure what the V.A. study argues. Again the central question was whether HIV causes AIDS, something the experience of the French hemophiliacs (and others) demonstrates to be the case. Do you think there is a single person in any branch of medicine that really believes HIV is not responsible for AIDS? If there is would they accept a transfusion with HIV in it? Would you? These are the salient questions, aren't they?
69
posted on
08/02/2008 5:30:01 PM PDT
by
count-your-change
(you don't have to be brilliant, not being stupid is enough.)
To: GodGunsGuts
Why are you bothering me with stuff that ASSUMES that HIV causes AIDS? Save that for the true believers.Why do you insist on hijacking my HIV/AIDS threads with rants about Duesberg and AZT toxicity, including old citations that used 1500 mg of AZT when today's maximum dose is 600 mg daily?
70
posted on
08/02/2008 6:14:12 PM PDT
by
neverdem
(I'm praying for a Divine Intervention.)
To: count-your-change
Don’t just sit on your hands. Take the time to read about the side effects of AZT. Hundreds of scientists and medical doctors are convinced this drug alone (not to mention all the other AIDS chemo drugs) killed tens to hundreds of thousands.
Side effects of AZT chemotherapy listed by category:
http://aras.ab.ca/azt.html
To: neverdem
I’m not hijacking anything. The thread is about AIDS, is it not? We are discussing AIDS, are we not? Are you getting frustrated because you are starting to sense that you might be on the losing side of the debate???
To: GodGunsGuts
Are you getting frustrated because you are starting to sense that you might be on the losing side of the debate???No, I'm frustrated with people like you spreading nonsense. And you never answered these questions from comment# 48 from this thread:
Deny the HIV to AIDS connection and you'll be attacked, crushed, and ruined
How do you explain the drop in new HIV/AIDS cases after blood was screened for HIV before transfusion of blood and blood products?
Why does giving antiretroviral drugs to HIV positive pregnant women just before and around the birth of their children reduce the rate of HIV positive children being born?
Why do HIV negative children breastfeeding from HIV positive mothers get AIDS and die from it?
Why do the highly active antiretroviral therapy(HAART) drugs decrease mortality and increase longevity?
As far as I'm concerned, Peter Duesberg has only one valid question - the diagnostic accuracy in Africa, but he ignores all of the good outcomes from using antiretroviral drugs there. He's fixated on homosexuals using amyl nitrate "poppers." Other than being a mind altering substance and less inhibited about being promiscuous, I don't see an explanation from Duesberg for why homosexuals get AIDS.
The same goes for intravenous drug abusers. They don't get AIDS if they use clean needles and don't share.(PERIOD!) And yes, they do exist. Not everyone is your typical junkie. Chronic alcoholics are more readily recognized for being immunocompromised.
73
posted on
08/02/2008 6:56:28 PM PDT
by
neverdem
(I'm praying for a Divine Intervention.)
To: GodGunsGuts
Like I said earlier, neither you nor any of those “hundreds of scientists and medical doctors’ would accept an injection containing the HIV.
See, I can cut to the heart of the matter even while sitting on my hands.
74
posted on
08/02/2008 7:43:28 PM PDT
by
count-your-change
(you don't have to be brilliant, not being stupid is enough.)
To: neverdem; count-your-change
==How do you explain the drop in new HIV/AIDS cases after blood was screened for HIV before transfusion of blood and blood products?
I already answered you in that same thread, but here it is again. Notice the exact opposite occured. During the time that they were screening blood for HIV, and the number of HIV positive blood donors began it precipitous decline, the number of AIDS cases continued to rise:
==Why does giving antiretroviral drugs to HIV positive pregnant women just before and around the birth of their children reduce the rate of HIV positive children being born?
Not "just" before birth, they are put on this drug for a full six months of their pregnancy. Should it come as any surprise that a DNA chain-terminator that randomly destroys rapidly dividing cells would reduce HIV transmission from mother to child? But as Duesberg notes, while AZT lowers transmission of HIV from mother to child by 17%, it comes at the cost of putting 100% of those same mothers on AZT CHEMOTHERAPY. And what of the side effects of the HIV-negative babies who are born from mothers who were put on prophylactic AZT? These babies suffer from "fevers, pneumonia, anemia, and mitochondrial dysfunction." And the reason should come as no surpise, given the exteme toxicity of AZT.
Label on AZT bottle:
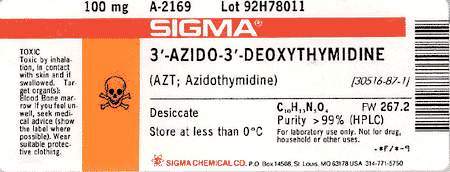
Label reads: "TOXIC. Toxic by inhalation, in contact with skin and if swallowed. Target organ(s): Blood bone marrow. If you feel unwell, seek medical advice (show the label where possible). Wear suitable protective clothing." Note that the bottle only contains 100mg. Pregant mothers are given 500mg.
Finally, take a look at the chart (I recreated it the best I could) from Duesberg's 2003 paper, complete with references. This would be bad enough if HIV was the cause of AIDS, but if Duesberg et al are correct, they are subjecting pregnant mothers/unborn babies to extremely toxic chemotherapy drugs, all in the name of preventing tranmission of a harmless retrovirus (HIV).
| Table 7. Diseases and mortality in HIV-free human babies, and in HIV-free animals treated with anti-HIV drugs before and after birth (BB, AB). |
| Species |
AIDS-defining |
Other disease |
References |
|
Human Babies (AB) Animals (AB): Mice, rats, dogs, monkeys Animals (BB) |
Fever, Pneumonia Lymphopenia, Weight loss, Leukemia, T-cell depletion, Thymic atrophy, Death of 25/30 mice Death |
Anemia, Mitochondrial dysfunction Anemia, neutropenia, Thrombocytopenia, Bone marrow depletion, Lymphotoxicity, Myelodysplasia, Muscle atrophy, Nephrotoxicity Hepatotoxicity Lung, liver, vaginal cancer Retarded development, Abortion |
(Blanche et al 1999), (Heresi et al 1997) (Ayers 1988; Cronkite and Bullis 1990; Thompson et al 1991; McKallip et al 1995; Omar et al 1996; Grossman et al 1997; Inoue et al 1997; Gerschenson et al 2000) (Toltzis et al 1993; Olivero et al 1997) |
To: neverdem; count-your-change; metmom; Stentor; Marty; Fractal Trader; DaveLoneRanger; Alamo-Girl; ...
(Thought the rest of you might be interested in this exchange...also see replies immediately above. All the best—GGG)
Almost forgot your last question:
==Why do the highly active antiretroviral therapy(HAART) drugs decrease mortality and increase longevity?
You couldn’t be more wrong about HAART chemotherapy. As it turns out, in 2006 the Lancet published a study of European and North American AIDS patients on HAART drugs (the largest of its kind, with hundreds of investigators listed). In the discussion section of the study the Lancet investigators admit the following with respect to AIDS cocktail/HAART drugs:
“However, there was no corresponding decrease in the rates of AIDS, or death, up to 1 year of follow-up. Conversely, there was some evidence for an increase in the rate of AIDS in the most recent period.”
http://www.duesberg.com/articles/2006,%20Lancet,%20HIV%20treatment%20resp..pdf
Now READ THIS. This study on HAART/(ART) therapy in Tanzania is nothing short of devestating to those in the AIDS establishment pushing these drugs on hapless Africans. The study is attached, but here are a few of its key points:
The cohort was 320 “treatment naive” patients placed on Anti-Retroviral Therapy (ART) between October 2003 and November 2006. Most (223) were women, some were as young as 15, the majority were between 25 and 34 years of age. Most were severely malnourished, had thrombocytopenia (low blood platelet count) and varying degrees of anemia.
Overall, 95 patients died, 59 of them within 3 months of starting the regimens.
From the paper:
“Conclusion: Mortality was found to be high, with the majority of deaths occurring within 3 months of starting ART. Anemia, thrombocytopenia and severe malnutrition were strong independent predictors of mortality. A prognostic model based on hemoglobin level appears to be a useful tool for initial risk assessment in resource-limited settings.”
...
One year mortality was estimated as high as 46.8% in those who were severely malnourished. This study states that other studies have confirmed the finding that severe malnutrition is correlated with death in HIV positive African patients “even after the introduction of highly active antiretroviral therapy...”
http://www.biomedcentral.com/1471-2334/8/52
The study goes on to say “There are some weaknesses of our study. First, mortality might be underestimated, since patients lost to follow-up probably include individuals dying at home without being reported.”
Needless to say, this study precisely matches what Duesberg has been saying all along re: African AIDS. African AIDS patients are primarily dying of malnutrition brought on by lack of food, not HIV. The HAART/ART drugs are simply killing them faster (and this will only intensify if the House version of Barack Obama’s global AIDS bill passes). The response to African AIDS should not be to put more Africans on chemotherapy. As Duesberg et al have always maintained, the surest and fastest way to cure African AIDS is to find a way to bypass their corrupt governments and FEED STARVING AFRICANS!
To: count-your-change
==Like I said earlier, neither you nor any of those “hundreds of scientists and medical doctors’ would accept an injection containing the HIV.
See, I can cut to the heart of the matter even while sitting on my hands.
Duesberg, Raznick, Ellison and several others have offered to do just that. All they require is that the NIH/CDC properly supervise the experiment, confirm that they have been injected with HIV and test positive for the same, and regularly report on their progress thereafter. In one other instance, Raznick offered to have himself injected without the above caveat, if the scientist he was debating at the time would agree to go on AIDS chemotherapy. At first, the scientist accepted the challenge, but later backed out.
To: allmendream
Any comments on the last half dozen or so replies???
To: GodGunsGuts
Those graphs have nothing to do with the decrease of new HIV/AIDS cases where the only risk factor was a transfusion of blood or blood product. They just show new increases in the total of all HIV/AIDS cases.
Not "just" before birth, they are put on this drug for a full six months of their pregnancy. Should it come as any surprise that a DNA chain-terminator that randomly destroys rapidly dividing cells would reduce HIV transmission from mother to child? But as Duesberg notes, while AZT lowers transmission of HIV from mother to child by 17%, it comes at the cost of putting 100% of those same mothers on AZT CHEMOTHERAPY. And what of the side effects of the HIV-negative babies who are born from mothers who were put on prophylactic AZT? These babies suffer from "fevers, pneumonia, anemia, and mitochondrial dysfunction." And the reason should come as no surpise, given the exteme toxicity of AZT.
It depends on the country, drug availability and choice of patient given their situation. I've read a few studies results where the drug or drugs were given for a minimum of a day or two antenatally and intrapartum. It works.
Public Health Service Task ForceRecommendations for Use of AntiretroviralDrugs in Pregnant HIV-Infected Women forMaternal Health andInterventions to Reduce Perinatal HIVTransmission in the United States
Panel’s Recommendations:Combination antepartum antiretroviral drug regimens are more effective than single-drug regimens in reducing perinatal transmission. • Longer duration of antepartum antiretroviral prophylaxis (e.g., starting at 28 weeks gestation) is more effective than shorter duration (e.g., starting at 36 weeks gestation); therefore, for women who do not require immediate initiation of therapy for their own health, prophylaxis should be started by 28 weeks gestation (see Recommendations for Use of Antiretroviral Drugs during Pregnancy). If women do not receive antepartum antiretroviral drugs, intrapartum combined with infant antiretroviral prophylaxis should be given to reduce the risk of perinatal transmission (see Intrapartum Care), although this is not as effective as when antepartum therapy is also given.If women do not receive antepartum or intrapartum antiretroviral drugs, postnatal infant antiretroviral prophylaxis is recommended with a minimum of 6 weeks of ZDV (see Postpartum Care).In the United States, the addition of single-dose intrapartum/newborn NVP to the standard antepartum combination antiretroviral regimens used for prophylaxis or treatment in pregnant women is not recommended because it does not appear to provide additional efficacy in reducing transmission and may be associated with the development of NVP resistance. • • • • July 8, 2008 5 Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States
Short-term efficacy has been demonstrated for a number of short-course antiretroviral regimens, including those with ZDV alone; ZDV plus 3TC; single-dose NVP; and more recently, combining single-dose NVP with either short-course ZDV or ZDV/3TC [14, 15, 17-24]. In general, combination regimens are more effective than single-drug regimens in reducing perinatal transmission, and when it's feasible and affordable, a longer 3-part regimen given antenatally, intrapartum, and postpartum is superior in preventing perinatal transmission than a shorter 2-part antepartum/intrapartum or intrapartum/postpartum regimen [15, 25, 26]
(split between pages 4 & 5 on the article, ending on page 10 of the Adobe page counter)
Copying text from pdf to html is problematic.
Adverse effects from zidovudine, AZT, are well known. That's probably why the daily dose is down to 600 mg.
79
posted on
08/02/2008 10:20:20 PM PDT
by
neverdem
(I'm praying for a Divine Intervention.)
To: neverdem
==Those graphs have nothing to do with the decrease of new HIV/AIDS cases where the only risk factor was a transfusion of blood or blood product. They just show new increases in the total of all HIV/AIDS cases.
Let me repeat the question you asked me: “How do you explain the drop in new HIV/AIDS cases after blood was screened for HIV before transfusion of blood and blood products?”
The graph clearly shows that AIDS cases continued their steep rise long after blood began being screened for HIV.
Navigation: use the links below to view more comments.
first previous 1-20 ... 41-60, 61-80, 81-100 ... 121-133 next last
Disclaimer:
Opinions posted on Free Republic are those of the individual
posters and do not necessarily represent the opinion of Free Republic or its
management. All materials posted herein are protected by copyright law and the
exemption for fair use of copyrighted works.
FreeRepublic.com is powered by software copyright 2000-2008 John Robinson