To: neverdem; count-your-change
==How do you explain the drop in new HIV/AIDS cases after blood was screened for HIV before transfusion of blood and blood products?
I already answered you in that same thread, but here it is again. Notice the exact opposite occured. During the time that they were screening blood for HIV, and the number of HIV positive blood donors began it precipitous decline, the number of AIDS cases continued to rise:
==Why does giving antiretroviral drugs to HIV positive pregnant women just before and around the birth of their children reduce the rate of HIV positive children being born?
Not "just" before birth, they are put on this drug for a full six months of their pregnancy. Should it come as any surprise that a DNA chain-terminator that randomly destroys rapidly dividing cells would reduce HIV transmission from mother to child? But as Duesberg notes, while AZT lowers transmission of HIV from mother to child by 17%, it comes at the cost of putting 100% of those same mothers on AZT CHEMOTHERAPY. And what of the side effects of the HIV-negative babies who are born from mothers who were put on prophylactic AZT? These babies suffer from "fevers, pneumonia, anemia, and mitochondrial dysfunction." And the reason should come as no surpise, given the exteme toxicity of AZT.
Label on AZT bottle:
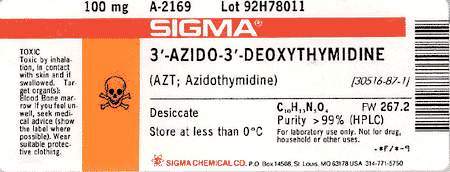
Label reads: "TOXIC. Toxic by inhalation, in contact with skin and if swallowed. Target organ(s): Blood bone marrow. If you feel unwell, seek medical advice (show the label where possible). Wear suitable protective clothing." Note that the bottle only contains 100mg. Pregant mothers are given 500mg.
Finally, take a look at the chart (I recreated it the best I could) from Duesberg's 2003 paper, complete with references. This would be bad enough if HIV was the cause of AIDS, but if Duesberg et al are correct, they are subjecting pregnant mothers/unborn babies to extremely toxic chemotherapy drugs, all in the name of preventing tranmission of a harmless retrovirus (HIV).
| Table 7. Diseases and mortality in HIV-free human babies, and in HIV-free animals treated with anti-HIV drugs before and after birth (BB, AB). |
| Species |
AIDS-defining |
Other disease |
References |
|
Human Babies (AB) Animals (AB): Mice, rats, dogs, monkeys Animals (BB) |
Fever, Pneumonia Lymphopenia, Weight loss, Leukemia, T-cell depletion, Thymic atrophy, Death of 25/30 mice Death |
Anemia, Mitochondrial dysfunction Anemia, neutropenia, Thrombocytopenia, Bone marrow depletion, Lymphotoxicity, Myelodysplasia, Muscle atrophy, Nephrotoxicity Hepatotoxicity Lung, liver, vaginal cancer Retarded development, Abortion |
(Blanche et al 1999), (Heresi et al 1997) (Ayers 1988; Cronkite and Bullis 1990; Thompson et al 1991; McKallip et al 1995; Omar et al 1996; Grossman et al 1997; Inoue et al 1997; Gerschenson et al 2000) (Toltzis et al 1993; Olivero et al 1997) |
To: GodGunsGuts
Those graphs have nothing to do with the decrease of new HIV/AIDS cases where the only risk factor was a transfusion of blood or blood product. They just show new increases in the total of all HIV/AIDS cases.
Not "just" before birth, they are put on this drug for a full six months of their pregnancy. Should it come as any surprise that a DNA chain-terminator that randomly destroys rapidly dividing cells would reduce HIV transmission from mother to child? But as Duesberg notes, while AZT lowers transmission of HIV from mother to child by 17%, it comes at the cost of putting 100% of those same mothers on AZT CHEMOTHERAPY. And what of the side effects of the HIV-negative babies who are born from mothers who were put on prophylactic AZT? These babies suffer from "fevers, pneumonia, anemia, and mitochondrial dysfunction." And the reason should come as no surpise, given the exteme toxicity of AZT.
It depends on the country, drug availability and choice of patient given their situation. I've read a few studies results where the drug or drugs were given for a minimum of a day or two antenatally and intrapartum. It works.
Public Health Service Task ForceRecommendations for Use of AntiretroviralDrugs in Pregnant HIV-Infected Women forMaternal Health andInterventions to Reduce Perinatal HIVTransmission in the United States
Panel’s Recommendations:Combination antepartum antiretroviral drug regimens are more effective than single-drug regimens in reducing perinatal transmission. • Longer duration of antepartum antiretroviral prophylaxis (e.g., starting at 28 weeks gestation) is more effective than shorter duration (e.g., starting at 36 weeks gestation); therefore, for women who do not require immediate initiation of therapy for their own health, prophylaxis should be started by 28 weeks gestation (see Recommendations for Use of Antiretroviral Drugs during Pregnancy). If women do not receive antepartum antiretroviral drugs, intrapartum combined with infant antiretroviral prophylaxis should be given to reduce the risk of perinatal transmission (see Intrapartum Care), although this is not as effective as when antepartum therapy is also given.If women do not receive antepartum or intrapartum antiretroviral drugs, postnatal infant antiretroviral prophylaxis is recommended with a minimum of 6 weeks of ZDV (see Postpartum Care).In the United States, the addition of single-dose intrapartum/newborn NVP to the standard antepartum combination antiretroviral regimens used for prophylaxis or treatment in pregnant women is not recommended because it does not appear to provide additional efficacy in reducing transmission and may be associated with the development of NVP resistance. • • • • July 8, 2008 5 Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States
Short-term efficacy has been demonstrated for a number of short-course antiretroviral regimens, including those with ZDV alone; ZDV plus 3TC; single-dose NVP; and more recently, combining single-dose NVP with either short-course ZDV or ZDV/3TC [14, 15, 17-24]. In general, combination regimens are more effective than single-drug regimens in reducing perinatal transmission, and when it's feasible and affordable, a longer 3-part regimen given antenatally, intrapartum, and postpartum is superior in preventing perinatal transmission than a shorter 2-part antepartum/intrapartum or intrapartum/postpartum regimen [15, 25, 26]
(split between pages 4 & 5 on the article, ending on page 10 of the Adobe page counter)
Copying text from pdf to html is problematic.
Adverse effects from zidovudine, AZT, are well known. That's probably why the daily dose is down to 600 mg.
79 posted on
08/02/2008 10:20:20 PM PDT by
neverdem
(I'm praying for a Divine Intervention.)
To: GodGunsGuts
“But as Duesberg notes, while AZT lowers transmission of HIV from mother to child by 17%, it comes at the cost of putting 100% of those same mothers on AZT CHEMOTHERAPY.”
But what explanation does Duesberg have for AZT lowering transmission of HIV from mother to child? What mechanism does he propose that avoids having AZT acting as an anti-retroviral? (inasmuch as Douchberg insists it is Chemotherapy).
92 posted on
08/03/2008 7:41:34 AM PDT by
allmendream
(If "the New Yorker" makes a joke, and liberals don't get it, is it still funny?)
To: GodGunsGuts
I already answered you in that same thread, but here it is again. Notice the exact opposite occured. During the time that they were screening blood for HIV, and the number of HIV positive blood donors began it precipitous decline, the number of AIDS cases continued to rise: That doesn't tell us much. The number of HIV positive blood donors can go down, while, at the same time, the number of AIDS cases continues to rise. Blood transfusions never accounted for more than a small percentage of AIDS cases. To support your position, you would have to show proof that even as the number of HIV positive blood donors went down, the rate of AIDs cases in people receiving blood transufusions continued to go up (controlling, of course, for other causes among such group such as male homosexuality or sharing needles). You can't do that since I'm going to bet that AIDS cases from blood tranfusions, at least in this country, are effectively zero.
121 posted on
08/04/2008 10:36:03 AM PDT by
Citizen Blade
("Please... I go through everyone's trash." The Question)
FreeRepublic.com is powered by software copyright 2000-2008 John Robinson