https://www.bbc.com/news/world-51235105
By this estimate, by about May 8th, all open hospital beds in the US will be filled. (This says nothing, of course, about whether these beds are suitable for isolation of patients with a highly infectious virus.)
If we’re wrong by a factor of two regarding the fraction of severe cases, that only changes the timeline of bed saturation by 6 days in either direction. If 20% of cases require hospitalization, we run out of beds by ~May 2nd.
If only 5% of cases require it, we can make it until ~May 14th. 2.5% gets us to May 20th. This, of course, assumes that there is no uptick in demand for beds from *other* (non-COVID19) causes, which seems like a dubious assumption.
As healthcare system becomes increasingly burdened, Rx shortages, etc, people w/ chronic conditions that are normally well-managed may find themselves slipping into severe states of medical distress requiring intensive care & hospitalization. But let’s ignore that for now.
Alright, so that’s beds. Now masks. Feds say we have a national stockpile of 12M N95 masks and 30M surgical masks (which are not ideal, but better than nothing).
There are about 18M healthcare workers in the US. Let’s assume only 6M HCW are working on any given day. (This is likely an underestimate as most people work most days of the week, but again, I’m playing conservative at every turn.)
As COVID19 cases saturate virtually every state and county, which seems likely to happen any day now, it will soon be irresponsible for all HCWs to not wear a mask. These HCWs would burn through N95 stockpile in 2 days if each HCW only got ONE mask per day.
One per day would be neither sanitary nor pragmatic, though this is indeed what we saw in Wuhan, with HCWs collapsing on their shift from dehydration because they were trying to avoid changing their PPE suits as they cannot be reused.
How quickly could we ramp up production of new masks? Not very fast at all. The vast majority are manufactured overseas, almost all in China. Even when manufactured here in US, the raw materials are predominantly from overseas...again, predominantly from China.
Keep in mind that all countries globally will be going through the exact same crises and shortages simultaneously. We can’t force trade in our favor.
Now consider how these 2 factors – bed and mask shortages – compound each other’s severity. Full hospitals + few masks + HCWs running around between beds without proper PPE = very bad mix.
HCWs are already getting infected even w/ access to full PPE. In the face of PPE limitations this severe, it’s only a matter of time. HCWs will start dropping from the workforce for weeks at a time, leading to a shortage of HCWs that then further compounds both issues above.
We could go on and on about thousands of factors – # of ventilators, or even simple things like saline drip bags. You see where this is going.
Importantly, I cannot stress this enough: even if I’m wrong – even VERY wrong – about core assumptions like % of severe cases or current case #, it only changes the timeline by days or weeks. This is how exponential growth in an immunologically naïve population works.
Undeserved panic does no one any good. But neither does ill-informed complacency. It’s wrong to assuage the public by saying “only 2% will die.” People aren’t adequately grasping the national and global systemic burden wrought by this swift-moving of a disease.
I’m an engineer. This is what my mind does all day: I run back-of-the-envelope calculations to try to estimate order-of-magnitude impacts. I’ve been on high alarm about this disease since ~Jan 19 after reading clinical indicators in the first papers emerging from Wuhan.
Nothing in the last 6 weeks has dampened my alarm in the slightest. To the contrary, we’re seeing abject refusal of many countries to adequately respond or prepare. Of course some of these estimates will be wrong, even substantially wrong.
But I have no reason to think they’ll be orders-of-magnitude wrong. Even if your personal risk of death is very, very low, don’t mock decisions like canceling events or closing workplaces as undue “panic”.
These measures are the bare minimum we should be doing to try to shift the peak – to slow the rise in cases so that healthcare systems are less overwhelmed. Each day that we can delay an extra case is a big win for the HC system.
And yes, you really should prepare to buckle down for a bit. All services and supply chains will be impacted. Why risk the stress of being ill-prepared? 28/n Worst case, I’m massively wrong and you now have a huge bag of rice and black beans to burn through over the next few months and enough Robitussin to trip out.
One more thought: you’ve probably seen multiple respected epidemiologists have estimated that 20-70% of world will be infected within the next year. If you use 6-day doubling rate I mentioned above, we land at ~2-6 billion infected by sometime in July of this year.
Obviously I think the doubling time will start to slow once a sizeable fraction of the population has been infected, simply because of herd immunity and a smaller susceptible population.
But take the scenarios above (full beds, no PPE, etc, at just 1% of the US population infected) and stretch them out over just a couple extra months. 32/n That timeline roughly fits with consensus end-game numbers from these highly esteemed epidemiologists. Again, we’re talking about discrepancies of mere days or weeks one direction or another, but not disagreements in the overall magnitude of the challenge.
This is not some hypothetical, fear-mongering, worst-case scenario. This is reality, as far as anyone can tell with the current available data.
That’s all for now. Standard disclaimers apply: I’m a PhD biologist but *not* an epidemiologist. Thoughts my own. Yadda yadda. Stay safe out there. /end
[[We’re looking at about 1M US cases by the end of April]]
Yeah, but who cares- mike bloomberg is gonna take $500 million of his own money and make every person a millionaire
(See previous article on FR about Brian Williams)
Well if it finally gets hospitals and insurance to actually charge realistic prices for procedures and meds, and stops them hiking up charges on your bill to cover nonpayers,
I say maybe this is the reset to the idiotic hcare system we have that we’ve all been waiting for.
[[Ms. Sprecht is right that people do not understand exponential growth. This is truly frightening information.]]
Been saying it for awhile now- We’re just in the very beginning stages right now, and people are getting all panicky about a few 1000 cases- IF this virus really takes off- the numbers will be in the millions- in a very short period- then people will really begin panicking- but that’s a big if-
BUT- let’s not forget, that viruses TEND TO burn themselves out pretty rapidly once they hit peak and begin declining in numbers of new cases- so it might not be too bad- Remember the bird flu? People panicked about that too- and while it was bad, it didn’t reach the pandemic levels that people were predicting
HOWEVER, that doesn’t mean that this virus won’t reach pandemic- it could- and if it does- it will very very rapidly get much worse, and there is no way we will ever be able to contain it- too many people can’t afford to take time off from work-
There are/won’t be enough hospital staff to keep hospitals running at
full occupancy. Hospital workers will refuse to come to work.
I’m not worried. If I get Corona Virus, I’ll just hook up with someone that has Lyme Disease.
and thanks for working out the math- gives a proper view of what ‘could happen’- were this virus to expand rapidly-
As far as ramping mask production up, the government has a contract with 3M to produce 36 million masks a month.
That’s not enough, but if the CV patients can be isolated from other patients, not all 18M healthcare workers will be needing masks. In fact a lot of them might never need to see a CV patient.
I’m sure 3M will be planning on more demand than just the feds. And I’m also sure other companies will be producing masks.
One of the ramifications of CV, might be stress on health insurance companies, unless the FED steps in an absorbs the cost.
If we did get 1,000,000 cases, and 15% of them needed hospitalization, that’s 150,000 cases at $1500/day
hospital stay for 3 weeks. That’s $675 million hit.
If the cost is $3000 that’s $1.3 Trillion. ICU is $4k a day.
Are health insurance companies going to go bankrupt?
Are they going to start denying care, because they just can’t pay?
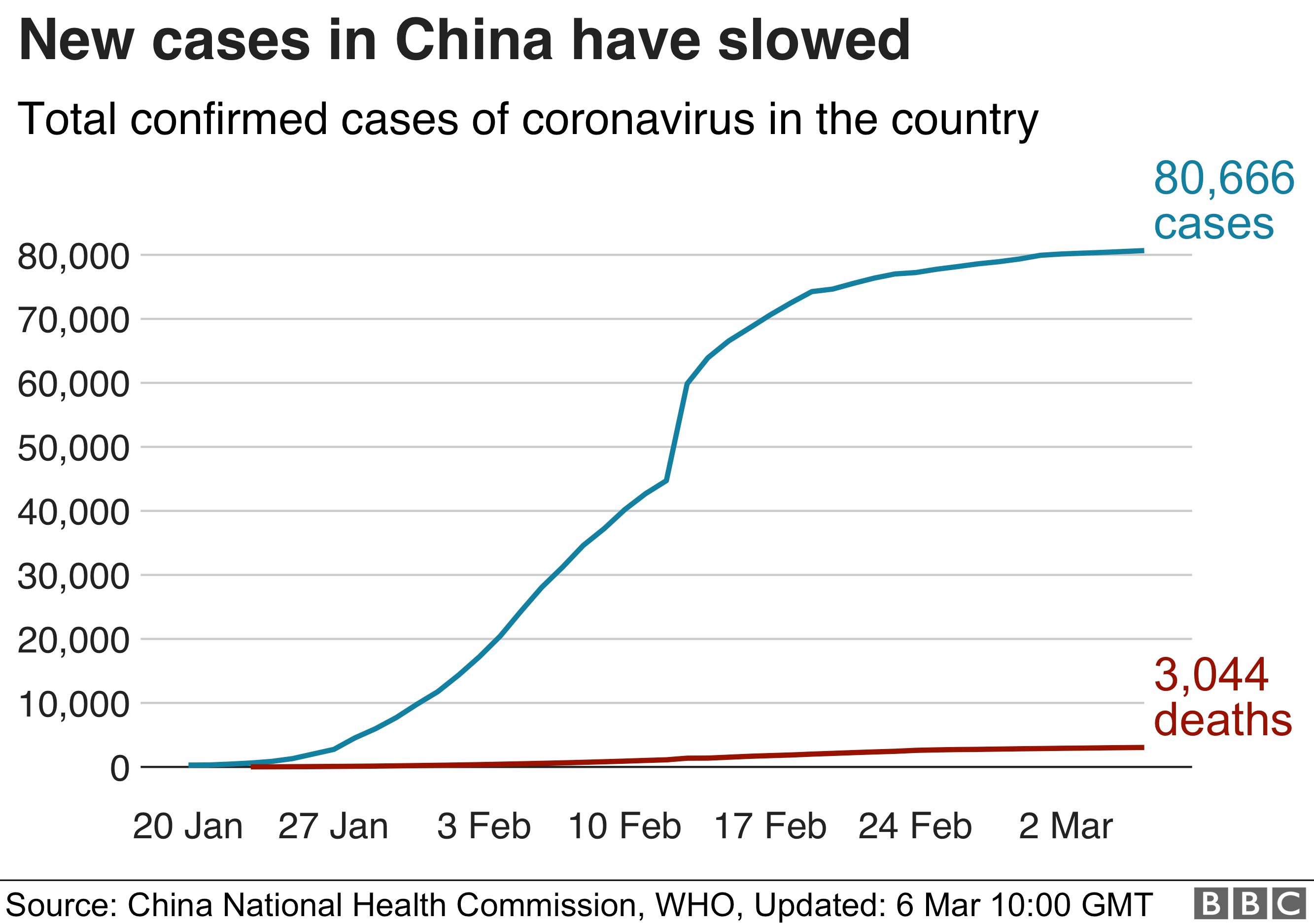
so are you of the opinion that China has not limited the virus spread over the past couple of weeks anywhere near as much as claimed?
Don’t listen to PhD biochemist who’s speciality is crap like the impossible whopper
Listen to the docs and nurses who have always been in the field
This woman is a loon. Her estimates are wildly over blown
Only critical patients should be in hospitals. The rest of all y’all stay home
Good hygiene. Hand washing. Call the doctor’s office if you don’t feel well. They will tell you what to do
When small pox was rampant in this country people quarantined in place. Health care still wasn’t the best. Even then the death rates weren’t what she’s claiming for this virus
Everybody needs to settle down and quit buying the media hype
My guess is lots of folks here going nuts about this virus didn’t get a flu shot or a pneumonia shot. They won’t get the vaccine against this either
You life in California. If I were you I’d be more concerned with TB and typhoid and others third world diseases
The growth rate in the USA doesn’t look scary to me so far. So far there are enough ventilators for the oldies.
Korea has some impressive growth but I think it’s a little deceptive because much of the numbers are because they have drastically expanded testing compared to everywhere else (drive through testing).
Iran looks like it could be really bad, scary growth rate.
I think that’s the one place other than China I’d be scared right now.
Don’t know what is really going on in China, not going to guess.
Italy looks like a real hot spot, maybe that could become bad or be a vector for other places. Nothing like Iran, but worse than everywhere else (other than China).
The other thing to consider is these viruses seem to always die down with moister air from summer. In rare cases there is a resurgance fall/winter.
The thing people have to consider is the possibility of viral mutation, where a new strain can change everything fast. Though most often these mutations just result in it dying off faster
This all is just my informal take, don’t know anything special just following the news casually.
The exponential multiplier should end at 14 days for the initial population or a total of 16,000. Also, as clusters occur in roughly the first 4 days the doubling will cease upon discovering the source and its connections so the doubling of infections will not last 14 days in any given area.
So because of limiting factors on exponential growth the model will find a stopping point as the number of new cases equals the number of recovers. With better testing and prevention this affected population will peak then subside.
Bookmark
LOL. If any of this were remotely true, the healthcare system would collapse 6 months out of every year just from influenza.
Interesting but I think you have forgotten a few things. While the existing supply of masks is “finite” (i.e. already made, boxed and either in a story, medical facility, or on its way), the manufacturing of masks is an ongoing process, and can even be run with 3 shifts or more depending on the supply of raw materials and trained workers.
In other words, production should eventually keep up with demand or even supersede it.
Another overlooked factor is the U.S. military. They have medical facilities on their bases (somewhat limited but available in times of emergencies, but our greatest logistical advantage is our ability to put major temporary field facilities up and ready to go in a very short period of time (i.e. Tent Cities with basic sanitation (i.e. outdoor latrines in isolated sections of the encampments) which are themselves in isolation from the general populace.
When the terrible earthquakes and tsunamis hit Indonedia, Ceylon (Sri Lanka), Thailand, possibly India, etc. about 10-15 years ago), our Navy put a whole U.S. city of 10,000 people in the area of the disasters near Indonesia in a matter of days. (Remember, an aircraft carrier can have a crew of up to 5,000 people).
We have a good number of aircraft carriers on various stations and some in ports for repairs or R&R. Other ships, esp. supply ships are also readily available to carry supplies to any coastal area of the US and its territories should the need arise to deliver anti-Virus supplies and health/living facilities for the people in heavily impacted areas (say Puerto Rico, Virgin Islands, coastal US states/cities/ports).
We have enough unoccupied land in the continental US to house hundreds of thousands of infected or suspected infected people (our deserts are vast, so are parts of Alaska, Texas, Wyoming/Montana, etc.)
My son’s Army Engineering company put up several major temporary and/or permanent bridges in a matter of hours while under fire in Iraq. The COE (Army), Seabees (old Navy engineers), and other specially trained military units could create major tent cities/facilities in a matter of hours upon reaching the designed holding areas. That is what they were trained for, and trained well at that.
We underestimate our ability to do miracles in a normal. everyday manner. I remember an old saying that goes roughly like this (from the military, possible Corps of Engineers or the Marines). “We can do the possible immediately; the impossible take’s a little bit longer”.
Thank God we have enough men and women in the military and health support agencies/facilities to take on a major disaster immediately. I would put my money on them any day.
Millenial snowflakes need not apply. You’d only get in the way of “real people”.
https://www.bbc.com/news/world-51235105
Exponential is what the layman doesn’t understand.
Remember the image from when people where still concerned about overpopulation? A jar has beans in it that divide into two every second. It takes ten years for the jar to be half full. How long does it take for the jar to become full?
Given that H1N1 ended up infecting 60 million, COVID 19 could easily top a few million cases within a year. The question is, how many of those would be mild vs. critical. And we don’t yet know how many strains there are.
Rando wingnut on Twitter:”This is not some hypothetical, fear-mongering, worst-case scenario. This is reality, as far as anyone can tell with the current available data.....That’s all for now. Standard disclaimers apply!!!!!!!!!!!”
Retard on FR: “boy this is like totally sciencz!”
I don’t know how to say this nicely but you are in a panic, it’s not your fault it often feels like the worst-case scenario is the only possible outcome...even though history consistently implores us not to think this way. Humans (and we engineers especially) are hard-wired to overreact to the negative while underplaying the positive that is what media repetition does. It’s like advertising. It impacts you whether you know it or not.
You are generating “facts” based on only worst case negative assumptions and a linear misinterpretation of data- that all evidence indicates is wrong. Yes, the virus will spread with a reproduction rate of 2.2 but the fatality rate is actually probably around 1%. As reported by New England Journal of Medicine. That is why no one worldwide under the age of 10 has died and the fatality rate for those under 40 is 0.2 % . Its why S Korea which after China reported the first cases and is reliably reporting numbers has 6,767 cases and 44 deaths or a fatality rate of .006, add the 52 critical and your fatality rate is .014 or 1.4% basically what the New England Journal of Medicine reported in a meta analysis of all. To see why read on.
As the New England Journal of Medicine reported
— The latest tally of almost 1,100 cases of COVID-19 infection from 30 Chinese provinces shows a fatality rate of 1.4% during the early phase of the outbreak.
That’s much higher than the rate seen with the seasonal flu, where only about 0.1% of cases end in death. But it’s far below the mortality rate of recent corona virus outbreaks like SARS (9 to 10%) or MERS (36%), noted Dr. Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases (NIAID).
Furthermore, the 1.4% figure cited in the new Chinese report, published Feb. 28 in the New England Journal of Medicine, is probably higher than the “real” death rate, Fauci added.
That’s because many corona virus cases are so mild they’re not even being reported, Fauci explained in an editorial he co-wrote in the same issue of the NEJM. Co-authors include Dr. Robert Redfield, who directs the U.S. Centers for Disease Control and Prevention, and Dr. Clifford Lane, deputy director of the NIAID.
“If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%,” Dr. Fauci and his colleagues explained.
“This suggests that the overall clinical consequences of COVID-19 may ultimately be more akin to those of a severe seasonal influenza pandemic [which has a case fatality rate of approximately 0.1%] or a pandemic influenza [similar to those in 1957 and 1968],” the experts wrote.
If you want to see the actual worldwide #s go to https://www.worldometers.info/coronavirus/#countries
Historically, the number of confirmed cases in various epidemics has tended to rise sharply for 8 to 10 weeks, then peaked. SARS (much more deadly) Ebola, MERS, ZEKA, Avian Flu, Swine Virus “Flu.
For SARS in 2003, ZIKA 2015, Swine virus aka Swine Flu 10 years ago the same negative assumptions were out there but they didn’t have the media fanning them every day as the payoff today is maybe it will slow the economy enough to defeat Trump-if you have any doubt about this see MSNBC smiling and gloating about how this can be Trump’s Katrina.
And while 80,000 died from the flu in 2018 (a bad year) there was very little panic as the media didn’t endlessly report on it.
Moderna and Regeneron, among others report that they already have a treatment (Regeneron who developed treatment for Ebola) ready for testing this summer-and you can expect it to be expedited-yes more sadly die-perhaps reach the level of 2018 flu and sadly it is primarily seniors who are compromised and they deserve our prayers not panic.