Posted on 10/29/2021 7:05:59 AM PDT by SoConPubbie
by Toby Rogers
Where to even begin with the FDA’s preposterous risk-benefit analysis of Pfizer’s mRNA COVID-19 “vaccine” in children ages 5 to 11?
Let’s start with my bona fides. I have a year of undergraduate statistics at one of the best liberal arts colleges in America (Swarthmore). I have a year of graduate statistics at the masters program rated #1 for policy analysis (UC Berkeley). And I have a Ph.D. in political economy from one of the top universities in the world (University of Sydney). My research focus is on corruption in the pharmaceutical industry so I’ve read scientific studies in connection with vaccines nearly every day for 5 years. Earlier in my career I worked professionally tearing apart shoddy cost-benefit analyses prepared by corporations that were trying to get tax breaks, contracts, and other concessions from local government. Suffice it to say I’ve thought a lot about risk-benefit analysis and I’m better equipped than most to read one of these documents.
The FDA’s risk-benefit analysis in connection with Pfizer’s Emergency Use Authorization (EUA) application to inject children ages 5 to 11 with their COVID-19 vaccine is one of the shoddiest documents I’ve ever seen.
Let’s take it from the top:
🚩 COVID-19 rates in children ages 5 to 11 are so low that there were ZERO cases of severe COVID-19 and ZERO cases of death from COVID in either the treatment (n= 1,518) or control group (n= 750). So any claims you see in the press about the Pfizer vaccine being “90% effective” in children are meaningless because they are referring to mild cases from which children usually recover quickly (and then have robust broad spectrum immunity). So there is literally no emergency in this population for which one could apply for Emergency Use Authorization. Pfizer’s application should be dead on arrival if the FDA actually followed the science and their own rules. We will return to this topic below.
🚩 Pfizer’s clinical trial in kids was intentionally undersized to hide harms. This is a well known trick of the pharmaceutical industry. The FDA even called them out on it earlier this summer and asked Pfizer to expand the trial and Pfizer just ignored them because they can. (Pfizer fudged it by importing data from a different study but this other study only monitored adverse outcomes for 17 days so if anything the new data polluted rather than clarified outcomes). To put it simply, if the rate of particular adverse outcome in kids as a result of this shot is 1 in 5,000 and the trial only enrolls 1,518 in the treatment group then one is unlikely to spot this particular harm in the clinical trial. Voilà “Safe & Effective(TM)”.
🚩 Pfizer only enrolled “participants 5-11 years of age without evidence of prior SARS-CoV-2 infection.” Does the Pfizer mRNA shot wipe out natural immunity and leave one worse-off than doing nothing as shown in this data from the British government? Pfizer has no idea because children with prior SARS-CoV-2 infection were excluded from this trial. This was by design. Toxic polluters have learned to not ask questions that they do not want the answers to, lest they wind up staring at their own smoking gun in a future court case.
According to an analysis by Alex Berenson:
“What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus. Specifically, vaccinated people don’t seem to be producing antibodies to the nucleocapsid protein, the shell of the virus, which are a crucial part of the response in unvaccinated people. This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE (or more than once, probably). It also means the virus is likely to select for mutations that go in exactly that direction because those will essentially give it an enormous vulnerable population to infect. And it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.”
🚩 Did Pfizer LOSE CONTACT with 4.9% of their clinical trial participants? The FDA risk-benefit document states: “Among Cohort 1 participants, 95.1% had safety follow-up ≥2 months after Dose 2 at the time of the September 6, 2021 data cutoff.” So what happened with those 4.9% who did not have safety follow-up 2 months after Dose 2? Were they in the treatment or control group? We have no idea because Pfizer isn’t saying. Given the small size of the trial, failing to follow up with 4.9% of the participants potentially skews the results.
🚩 The follow up period was intentionally too short. This is another well-know trick of the pharmaceutical industry designed to hide harms. Cohort 1 appears to have been followed for 2 months, cohort 2 was only monitored for adverse events for 17 days. Many harms from vaccines including cancer and autoimmune disorders take much longer to show up. As the old saying goes, “you can have it quick or you can have it done right, but you cannot have both.” Pfizer chose quick.
🚩 The risk-benefit model created by the FDA only looks at one known harm from the Pfizer mRNA shot — myocarditis. But we know that the real world harms from the Pfizer mRNA shot go well beyond myocarditis and include anaphylaxis, Bell’s Palsy, heart attack, thrombocytopenia/ low platelet, permanent disability, shingles, and Guillain-Barré Syndrome (GBS) to name a few. Cancer, diabetes, endocrine disruption, and autoimmune disorders may show up later. But the FDA does not care about any of that because they have a vaccine to sell so they just ignore all of those factors in their model.
🚩 Pfizer intentionally wipes out the control group as soon as they can by vaccinating all of the kids who initially got the placebo. They claim that they are doing this for “ethical reasons”. But everyone knows that Pfizer’s true aim is to wipe out any comparison group so that there can be no long term safety studies. Wiping out the control group is a criminal act and yet Pfizer, Moderna, J&J, and AZ do this as standard practice with the blessing of the FDA/CDC.
🚩 Given all of the above, how on earth did the FDA claim any benefits at all from this shot? You should probably sit down for this part because it’s a doozy! Here’s the key sentence:
Vaccine effectiveness was inferred by immunobridging SARS-CoV-2 50% neutralizing antibody titers (NT50, SARS-CoV-2 mNG microneutralization assay).
Wait, what!? I’ll explain. There were ZERO cases of severe COVID-19 in the clinical trial of children ages 5 to 11. So Pfizer and the FDA just ignored all of the actual health outcomes (they had to, there is no emergency, so the application is moot). INSTEAD Pfizer switched to looking at antibodies in the blood. In general, antibodies are a poor predictor of immunity. And the antibodies in the blood of these 5 to 11 year old children tell us nothing because again, there were zero cases of severe COVID-19 in this study (none in the treatment group, none in the control group). So Pfizer had to get creative! What they came up with is “immuno-bridging”. Pfizer looked at the level of antibodies in the bloodwork of another study, this one involving people 16 to 25 years old, figured out the level of antibodies that seems to be protective in that population, then figured out how many kids ages 5 to 11 had similar levels of antibodies in their blood, and then came up with a number for how many cases, hospitalizations, ICU admissions, and deaths would be prevented by this shot in the 5 to 11 population in the future, based on the antibody levels and health outcomes from the 16 to 25 year old population. If your head hurts from that tortured logic, it should, because such chicanery is unprecedented in a risk-benefit analysis.
So when the FDA uses this tortured logic at the beginning of their briefing document, all of the calculations that stem from this will be flat out wrong. Not just wrong but preposterous and criminally wrong.
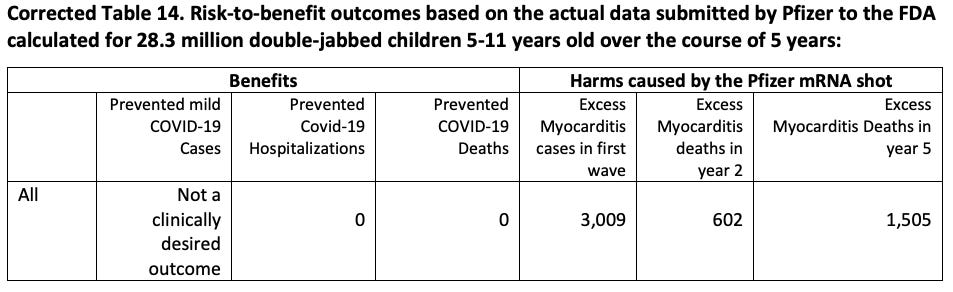
The whole ballgame comes down to Table 14 on page 34 of the FDA’s risk-benefit document. And there the red flags come fast and furious.
🚩 The FDA model only assesses the benefits of vaccine protection in a 6-month period after completion of two doses. Furthermore it assumes constant vaccine efficacy during that time period. This is problematic on several counts.
First, reducing mild cases in children is not a desired clinical outcome. As Dr. Geert Vanden Bossche points out, mass vaccination turns kids into shedders of more infectious variants.
“Under no circumstances should young and healthy people be vaccinated as it will only erode their protective innate immunity towards Coronaviruses (CoV) and other respiratory viruses. Their innate immunity normally/ naturally largely protects them and provides a kind of herd immunity in that it dilutes infectious CoV pressure at the level of the population, whereas mass vaccination turns them into shedders of more infectious variants. Children/ youngsters who get the disease mostly develop mild to moderate disease and as a result continue to contribute to herd immunity by developing broad and long-lived immunity. If you are vaccinated and get the disease, you may develop life-long immunity too but why would you take the risk of getting vaccinated, especially when you’re young and healthy? Firstly, there is the risk of potential side effects; secondarily, there is the ever increasing risk that your vaccinal antibodies will no longer be functional while still binding to the virus, thereby increasing the likelihood of ADE or even severe disease….”
Second, we know that vaccine efficacy in the month after the first dose is negative because it suppresses the immune system and it begins to wane after 4 months so all of the FDA’s estimates of vaccine efficacy are inflated.
Third, the harms of myocarditis from these shots will likely unfold over the course of years. Robert Malone, the inventor of mRNA technology notes that the FDA is admitting that children will be injected twice a year forever (hence the six month time frame in the FDA risk-benefit model). But the risks of “adverse events such as cardiomyopathy will be cumulative.” So any model that only looks at a six month time frame is hiding the true adverse event rate.
🚩 The FDA/Pfizer play fast and loose with their estimates of myocarditis. First they estimate “excess” (read: caused by the shot) myocarditis using data from the private “Optum health claim database” instead of the public VAERS system (p. 32). So it’s impossible for the public to verify their claims. Then, when it comes to estimating how many children with vaccine-induced myocarditis will be hospitalized and admitted to the ICU they use the Vaccine Safety Datalink (see page 33). Why switch to a different database for those estimates? Finally, there is no explanation for how they calculated “excess” myocarditis deaths, so they just put 0. Red flag, red flag, red flag.
The FDA estimates that there will be 106 extra myocarditis cases per 1 million double-jabbed children 5-11. There are 28,384,878 children ages 5 to 11 in the U.S. The Biden administration wants to inject Pfizer mRNA shots into all of them and has already purchased enough doses to do just that (even though only 1/3rd of parents want to jab their kids with this shot). So (if the Biden administration has its way) 106 excess myocarditis cases per 1 million x 28.38 million people would be 3,009 excess myocarditis cases post-vaccination if the Pfizer vaccine is approved.
And over the course of several years many of those children will die. Dr. Anthony Hinton (“Consultant Surgeon with 30 years experience in the NHS”) points out that myocarditis has a 20% fatality rate after 2 years and a 50% fatality rate after 5 years.
Viral myocarditis results in 2 in 10 people dead after 2 years and 5 in 10 after 5 years. It’s not mild. It’s dead heart muscle. https://t.co/ixRmk48rja
— Dr Anthony Hinton (@TonyHinton2016) October 20, 2021
So the FDA has it exactly backwards — they want to prevent mild COVID in children which reduces herd immunity and they just flat out lie about the harms from myocarditis.
I’ve taken the liberty to correct the FDA’s Table 14 with actual real world data and extended it over 5 years. It looks like this:
A study by Harvard Pilgrim Healthcare for the U.S. Department of Health and Human Services estimated that VAERS only captured 1% of actual vaccine injuries. Steve Kirsch has done elaborate modeling that puts the Under-Reporting Factor of COVID-19 vaccine deaths at 41 (so multiply the above numbers by 41). And myocarditis is just one of a multitude of possible harms from COVID-19 vaccines. Dr. Jessica Rose recently calculated an Under-Reporting Factor of 31 for all severe adverse events following vaccination.
Conclusion
The Pfizer vaccine fails any honest risk-benefit assessment in connection with its use in children ages 5 to 11. The FDA’s risk-benefit analysis of Pfizer’s mRNA vaccine in children ages 5 to 11 is shoddy. It used tortured logic (that would be rejected by any proper academic journal) in order to reach a predetermined result that is not based in science. The FDA briefing document is a work of fiction and it must be withdrawn immediately. If the FDA continues with this grotesque charade it will cause irreparable harms to children and the FDA leadership will one day be prosecuted for crimes against humanity.
[Updated to add:]
🚩 An astute reader pointed out that on page 14, the FDA explains that Pfizer has changed the ingredients in their mRNA vaccine. They write:
To provide a vaccine with an improved stability profile, the Pfizer-BioNTech COVID-19 Vaccine for use in children 5-11 years of age uses tromethamine (Tris) buffer instead of the phosphate-buffered saline (PBS) as used in the previous formulation and excludes sodium chloride and potassium chloride.
I’m deeply skeptical of this account (I doubt this has anything to do with an “improved stability profile”) and invite others to weigh in on this. I also recall that tromethamine has a long and troubled history and invite readers to dig into this further (I’m happy to post additional links as they become available).
This is a live article. The FDA only gives the public 2 days to review meeting materials so I had to publish this article immediately. If you spot any errors please let me know and I will correct them. If you find additional flaws in the FDA’s risk-benefit analysis please post them in the comments so that I may add them.
A revolution is coming.
Published with permission of the author
P
The government is trying to silence America’s Frontline Doctors.
The End of the Gentile Age
“And this Gospel shall be proclaimed to all the nations...and then the End will come.”
“Why do the heathen rage and plan a vain thing against Yaweh and His Annointed Jeshua”
Psalm 2
📌
“And Yaweh Theo shall send them a strong delusion”
2 Thessalonians
The liability that Big Pharma has received from Congress needs to be reassigned to (deducted from) Congressional salaries.
This is simply another war crime in progress. We should be getting used to these by now.
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.