Posted on 03/27/2020 4:49:42 AM PDT by Kaslin
Many in the media enthusiastically relish the claim that the United States has more people infected with the coronavirus than China does, even though China's numbers are unreliable.
When Donald Trump tweeted this week that the United States had performed more coronavirus tests than any other country, the media were upset.
Trump being Trump, he’d also said the United States had done more tests in eight days than South Korea had done in eight weeks. PolitiFact calculated the United States had done 17,582 fewer tests than South Korea during that time period. LiveScience said the United States had done 43,790 fewer tests than South Korea during that time period.
Their own disparity notwithstanding, other media outlets pointed out merely that South Korea is a much smaller country than the United States. That meant they had done more tests per capita than the United States had.
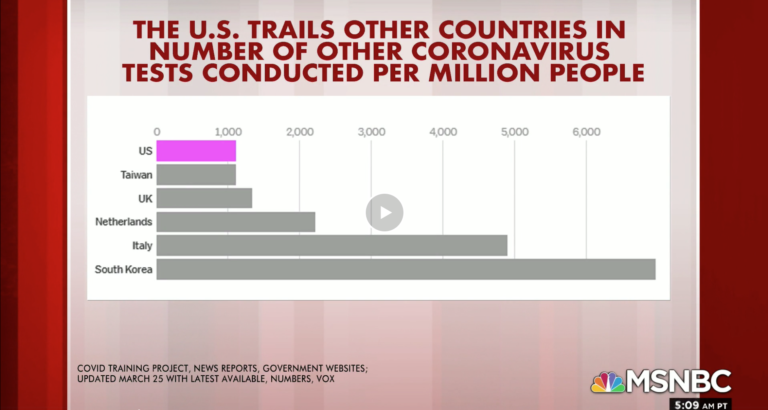
“Trump overlooks a huge piece of context,” a USA Today fact check said. CNN went with “Fact Check: US has done more coronavirus tests than South Korea, but not per person.” MSNBC ran a segment with a graph asserting that “The U.S. Trails Other Countries In Number Of Other Coronavirus Tests Conducted Per Million People.”
The segment is utterly wild, incidentally. You can watch it here, but while Mika Brzezinski moans and grunts in agreement, Joe Scarborough accuses the president of “lying” and says you have to adjust for population because of “science.” As if speaking to Trump, he says, “This is science. I don’t know … maybe you didn’t take … science at whatever school your daddy got you into. I don’t know. But this is just science.”
While the media have been doing a demonstrably bad job covering the coronavirus and the administration — and have the sinking poll numbers to prove it — this is a good point. Numbers should be placed in context. Comparing countries of different size by aggregate numbers isn’t particularly helpful.
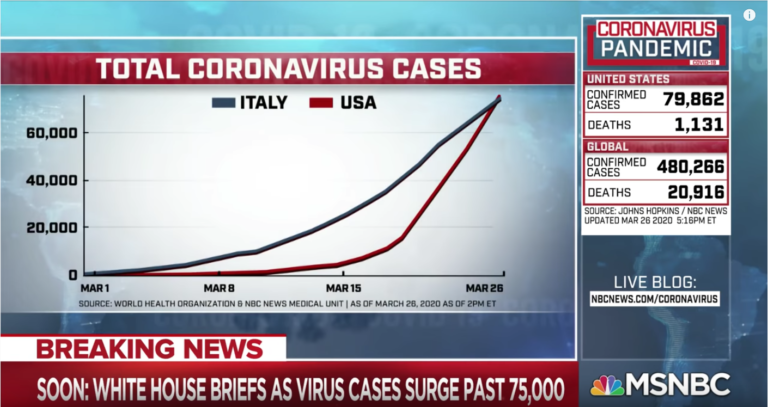
Yet that’s what happens all the time. For example, just a couple of hours after Scarborough’s “science” rant, his colleague Chuck Todd began his show by comparing the United States’s coronavirus cases with Italy’s, even though the United States has a much larger population, and the number of cases has something to do with the number of tests being conducted, and the United States has conducted more tests than any other country has:
CNN, which just days ago praised the need for per capita comparisons, tweeted this last night:
Italy is much smaller than the United States, China is much bigger.
Speaking of China and their reported cases, there is also the issue of the quality of China’s reporting. China claims that it arrested the spread of the virus overnight a few weeks ago. It skyrocketed up to 80,000 cases and then just stopped spreading in China and began spreading everywhere else in the world.
Even with their draconian measures of welding people into their apartments, forbidding travel, electronic surveillance of the affected, and other measures, these numbers are impossible to believe. As Jeryl Bier points out, the last paragraph of a New York Times article is reported credulously when it shouldn’t be: “China’s National Health Commission said earlier on Thursday that all 67 new coronavirus cases officially reported across the country on Wednesday were people who had been infected overseas, as were all 47 reported the previous day.”
As the reported cases in the United States surpassed the reported cases in China — not difficult to do given China’s very low quality of reporting and the fact that the United States is doing more testing than any other country — media were sure to trumpet the numbers:

Yet many in the media don’t just believe them but enthusiastically relish the claim that the United States has more people infected with the coronavirus than China does. Joe “Science Means You Have To Always Do Per Capita Comparisons” Scarborough weighed in:

Many media figures gave Chinese propagandists a run for their money. Here, frequent CNN guest Julia Ioffe said, of a country that is full of public health officials and doctors working valiantly to tackle a global epidemic, that it is a “s—hole” country.
Julia, you might recall, has had a rough couple of years, including tweeting her speculative fantasies about Trump involving incest, falling hard for debunked Russia collusion hoaxes, and being pretty sure she’d figured out an elaborate Russian plot regarding Hunter Biden’s indiscretions.
Ioffe’s fellow Russia collusion hoax promoter Benjamin Wittes was similarly excited by the increase in recorded cases of the deadly virus among his fellow Americans:
Again, sounding like Communist Chinese propagandists, media outlet The Verge renamed the Wuhan Virus the American Virus on account of U.S. testing and results:

Nobody in the media has explained why they accept the Communist Chinese government’s reported numbers despite their track record. As for whether to report numbers that are or are not controlled for population, even that metric can be lacking.
For instance, while Washington state had the earlier significant outbreak of the novel Chinese Coronavirus, New York is experiencing much worse spread. Further, in the United States of America, each state has the right to respond differently to the outbreak. It is more worthwhile to compare by city.
Not everyone was bad on this point. The Washington Examiner’s Phil Klein put many of the global numbers in context for his article, “US does not have close to the most coronavirus cases when adjusted for population.” Also, credit to Jim Geraghty for his ongoing skepticism of Communist Chinese propaganda.

Do you believe him?
The “Case Fatality Rate” in New York state is 1.2%.
The CFR in New York City is 1.6%.
The CFR for the entire USA is 1.5%. That rate has been steady or slightly falling for three straight weeks.
To put someone on a vent you have t intubate them. I certainly have never seen anyone try something else and i imagine if you tried there would be so many leaks you wouldn’t even be ventilating the patient. You. Would be ventilating the room.
The best stat I saw for was the one showing 21 million fewer cell phone subscribers. Where did they go? Hmmmmmm....
Look at the # new deaths in NYC. I imagine they are getting a lot of practice at intubation.
Whereas patients put on ventilators who did not require intubation had a slightly higher survival rate, with only 92% dying.
THAT's a relief!!
But really; how long do they LIVE before they finally die?
indeed, the city is going to be banking on tax sales. by the way their profit should be given back to families... imagine mortgage insurers doingthat
I ran ICUs for 5 months of my surgical internship. Not quite on the “DeBake model” but close. 15 beds and at times almost all of them on vents. In my younger days I was quite good at it because when you are managing a child with a brain tumor on a vent if you don’t know what the hell. You are doing you will kill them quickly.
They switched carriers to get a pair of new Iphones and got scammed outta their old ones.
People are frightened. They don’t understand what is happening and they want answers. That’s no reason to be rude.
To put someone on a vent you have t intubate them. I certainly have never seen anyone try something else and i imagine if you tried there would be so many leaks you wouldn’t even be ventilating the patient. You. Would be ventilating the room.
I'm a complete layman, but this is an elaboration of what I've read about non-invasive ventilation:
Mechanical ventilation is the most widely used supportive technique in intensive care units. Several forms of external support for respiration have long been described to assist the failing ventilatory pump, and access to lower airways through tracheostomy or endotracheal tubes had constituted a major advance in the management of patients with respiratory distress. More recently, however, new “noninvasive” ventilation (NIV) techniques, using patient/ventilator interfaces in the form of facial masks, have been designed.
The reasons for promoting NIV include a better understanding of the role of ventilatory pump failure in the indications for mechanical ventilation, the development of ventilatory modalities able to work in synchrony with the patient, and the extensive recognition of complications associated with endotracheal intubation and standard mechanical ventilation.
NIV has been used primarily for patients with acute hypercapnic ventilatory failure, and especially for acute exacerbation of chronic obstructive pulmonary disease. In this population, the use of NIV is associated with a marked reduction in the need for endotracheal intubation, a decrease in complication rate, a reduced duration of hospital stay and a substantial reduction in hospital mortality. Similar benefits have also been demonstrated in patients with asphyxic forms of acute cardiogenic pulmonary oedema. In patients with primarily hypoxemic forms of respiratory failure, the level of success of NIV is more variable, but major benefits have also been demonstrated in selected populations with no contraindications such as multiple organ failure, loss of consciousness or haemodynamic instability.
One important factor in success seems to be the early delivery of noninvasive ventilation during the course of respiratory failure. Noninvasive ventilation allows many of the complications associated with mechanical ventilation to be avoided, especially the occurrence of nosocomial infections. The current use of noninvasive ventilation is growing up, and is becoming a major therapeutic tool in the intensive care unit.
Without mechanical support for respiration, many patients would die within hours to days due to acute hypoxaemic and hypercapnic respiratory failure. Observational, physiological and case/control studies form a large body of evidence demonstrating that noninvasive ventilation (NIV) can be used in many situations to decrease a patient's dyspnoea and work of breathing, improve gas exchange and ultimately avoid the need for endotracheal intubation (ETI) 1–3. Randomised controlled trials have confirmed this and helped delineate when NIV should be used as a first-line treatment. Studies conducted outside the context of clinical trials are also of great importance in ensuring that the results of these trials can be obtained in real life 4–6. Indeed, the success of NIV may follow a learning curve, and early results may not be as good as those obtained later. In addition, it must be clear to clinicians that NIV is a complementary technique and cannot replace ETI in all instances.
In theory, the modes and settings for the delivery of NIV could be very similar to those for traditional mechanical ventilation through an endotracheal tube or tracheotomy cannula. In practice, because the circumstances of ventilation are different, the population of patients more selected and the equipment available sometimes more limited, this is not the case. In addition, leaks are a quasiconstant feature of NIV 7, 8. NIV is usually delivered in the form of assisted ventilation, in which every breath is supported by the ventilator. Rarely, controlled mechanical ventilation is used.
[To put someone on a vent you have t intubate them. I certainly have never seen anyone try something else and i imagine if you tried there would be so many leaks you wouldn’t even be ventilating the patient. You. Would be ventilating the room.]
This is going to get technical. If you subject tissue to more than ten # PSI you stop the capillary blood flow. If you try to use a mask to stop the leaks you have to inflate the seal to 10 lbs PSI because to keep the alveoli open you need 5 cm of Positive End Expiratory Pressure or PEEP. Which is about 5 lbs. to prevent leaks. This is not a new idea. It was tried 30 years ago. Occluding the capillaries under the seal for a day or two causes necrosis of parts of the face and then the seal is lost anyway. Sorry to rain on your parade.
I haven’t seen a copy of The Lancet study. All I have is an IPad and a router. I will say this, Lancet has an excellent reputation and if they published it you can generally take it to the bank. Unlike that ridiculous email that some (adjective deleted) was spamming everywhere a couple days ago. When I can stumble across it, believe me I will be reading it.
Here is what I have been saying. It is probably too late to start blue people on meds. It is probably over treating to put everybody who tests positive on drugs. So who do we put on drugs, even if they work to some extent? Everyone admitted to the hospital? Maybe. It would be logical. But first I still want to know that there were no or few people on Plaquenil prior who are among the Dead and seriously ill. Putting people who are critically ill on a drug we don’t have a real good idea works clinically could be a real mistake.
And any. Body who says they took it for months in Viet Nam, you were 18 and healthy as a horse. You probably could have taken small doses of cyanide.
Lancet is one of those Journals you don’t have to look for the red flags first. They have good editors.
[This is going to get technical. If you subject tissue to more than ten # PSI you stop the capillary blood flow. If you try to use a mask to stop the leaks you have to inflate the seal to 10 lbs PSI because to keep the alveoli open you need 5 cm of Positive End Expiratory Pressure or PEEP. Which is about 5 lbs. to prevent leaks. This is not a new idea. It was tried 30 years ago. Occluding the capillaries under the seal for a day or two causes necrosis of parts of the face and then the seal is lost anyway. Sorry to rain on your parade.]
People are being absolutely buried in bull shit. Which is why I have been here every day trying to help.
Experience. It is why you want to keep a few old people around.
[Putting people who are critically ill on a drug we don’t have a real good idea works clinically could be a real mistake.]
Disclaimer: Opinions posted on Free Republic are those of the individual posters and do not necessarily represent the opinion of Free Republic or its management. All materials posted herein are protected by copyright law and the exemption for fair use of copyrighted works.