To: momincombatboots
This simply is not true.
1. Peep of +10 to start no one in my treatments have required PEEP of +15. It would be malpractice to dial in a PEEP of +25. He loses all credibility there. If you were to use a High PEEP he would if legit have used APRV ventilations
2. Prolonged qT is not a wide ranging side effect. He is trying to throw some shade at a testament protocol
3. The combination of Plaquenil and azithromycin in almost all studies is showing significant benefit. See French study of yesterday. Most lall
Hospitals in America are using thise combo. For my critical care unit PUI are place on this combination. For those who test (+) we are seeing either failure to progress to vent or coming off the vent more quickly.
4. He is incorrect in the anectdoatal RLL statement. Any basic medical students knows this is an aspiration finding. There was an article a few days ago which this post place rises that said something about this. Most radiologists and clinicians will tell you if there is a favored love its the bilateral upper lines
5. He fails to mention prone ventilation. Anyone who is serious would probe a patient well before a PEEP of +25
I am so sorry to poly out this is an unsourced internet plate risk that has spread from several sources and is not consistent with any clinical expertise. The above five errors are glaring. People want to believe what they want to believe I guess. But this is incorrect. There is worldwide data softening bother the scope and severity of this virus. We are getting a far better handle on who it affects and why. We have valid and decent treatment options that will continue to be used. It’s easy to amass a bunch of internet things and work it into a well written though totally incorrect document such as this
If you want to be scared then be scared but please stop spreading incorrect clinical information. The real ER docs deserve much better than this
47 posted on
03/29/2020 5:12:10 AM PDT by
gas_dr
(Trial lawyers AND POLITICIANS are Endangering Every Patient in America)
To: gas_dr
Comparing Flu and COVID-19 deaths. Today, 07:41 PM by Ronan Kelly, FluTrackers
For the past several years, I have been plotting and comparing week to week influenza mortality data gathered by the National Center for Health Statistics (NCHS) mortality surveillance system. The number of coded flu deaths per year is only a part of the estimated flu deaths each week. I added US coronavirus deaths by week to the plot and got this:
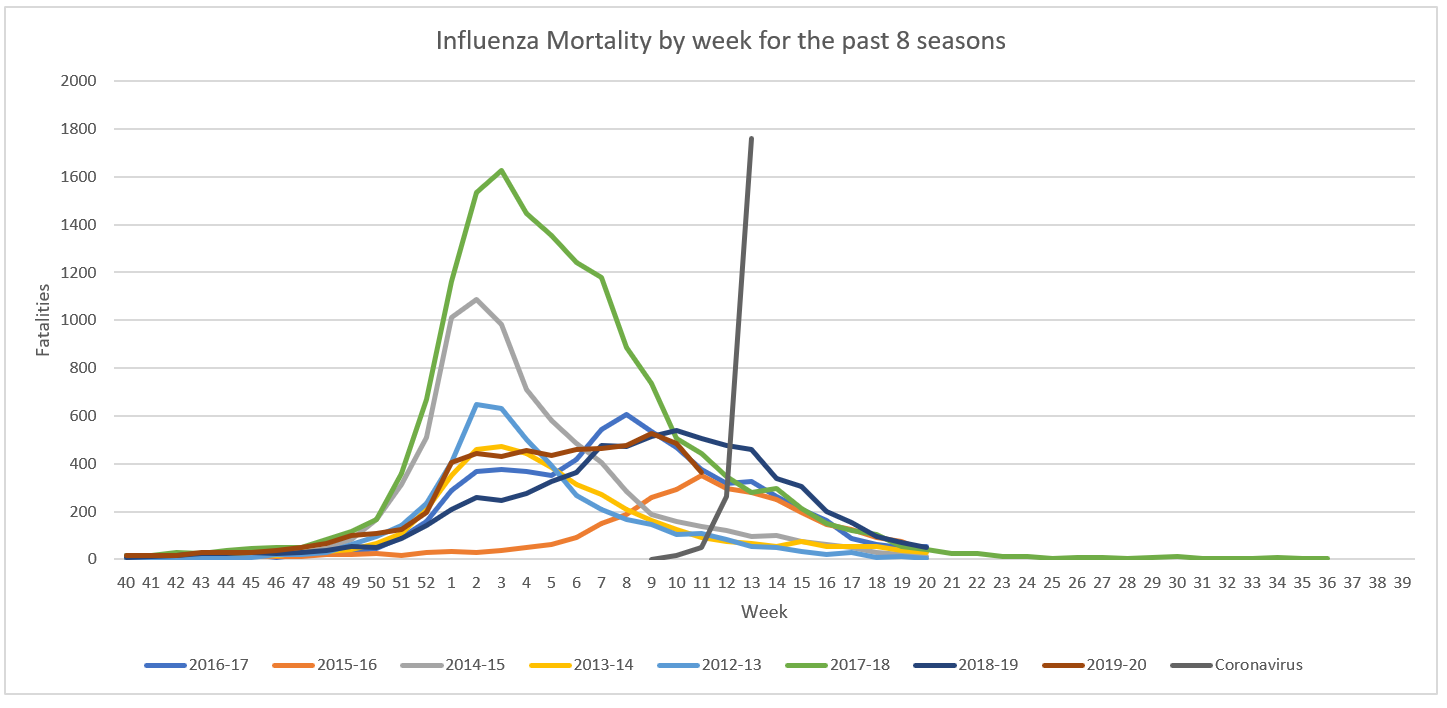
I know it's not apples to apples, the estimated number of flu deaths is about 6 times higher than the numbers recorded by the NCHS, but there is every reason to believe that the actual number of coronavirus fatalities is also larger than the subset that gets confirmed. There has only been 4 weeks of data. Where is this going to end up? https://flutrackers.com/forum/forum/-2019-ncov-new-coronavirus/united-states-2019-ncov/842586-comparing-flu-and-covid-19-deaths#post842586
53 posted on
03/29/2020 5:15:57 AM PDT by
Travis McGee
(EnemiesForeignAndDomestic.com)
To: gas_dr; momincombatboots
Your detailed assessment is appreciated, gas_dr.......
it serves to underline the multiple exasperating manifestations of the virus.
The author's experiences are as valuable as those that other medics are experiencing.
62 posted on
03/29/2020 5:20:45 AM PDT by
Liz
(Our side has 8 trillion bullets; the other side doesn't know which bathroom to use.)
To: gas_dr
My sister had a bad case of pneumonia and was vented for a couple of weeks. She barely made it. She was in an induced coma for a bit. I watched the doctors and therapists and what they did with the vent settings. It seemed a mix of science and art. Lost of blood work and adjusting. O2 settings and pressure and pace. Amazing machine and people that run them. Saved my sister.
To: gas_dr
Re: 47 - Thank you for posting this.
70 posted on
03/29/2020 5:24:01 AM PDT by
Fury
To: gas_dr
Funny how so many decry evidence as “anecdotal” and then use anecdotal observations when they fit their argument.
BTW, this post went viral about 4 days ago. The doc goes by the handle of “nawlinsag”. Source of post was at site called “texasags.com”.
I looked at some of his other posts and he appears legit, but your expertise could probably tell better. But he didn’t give near enough info on patient conditions when treated, how many, dosage, deaths after treatment, etc.
To: gas_dr
If he is using laminar flow the PEEP may be the highest pressure the lungs “see”. We used to get patients like this and in those days they just died.
104 posted on
03/29/2020 5:46:31 AM PDT by
wastoute
(Government cannot redistribute wealth. Government can only redistribute poverty.)
To: gas_dr
Doc, have a look at Cytosorbents Co. Blood filtration cartridges (Hooks up to existing dialysis equip.) for your CV Sepsis / Cytokine Storm patients. “Compassionate use” protocol. Was / is being used in China and now Italy.
110 posted on
03/29/2020 5:48:41 AM PDT by
DAC21
( and Naflet had demint)
To: gas_dr
5. He fails to mention prone ventilation. Anyone who is serious would probe a patient well before a PEEP of +25 From the article:
"Proning vented patients significantly helps oxygenation. Even self proning the ones on nasal cannula helps."
155 posted on
03/29/2020 6:16:44 AM PDT by
null and void
(By the pricking of my lungs, Something wicked this way comes ...)
FreeRepublic.com is powered by software copyright 2000-2008 John Robinson